

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Behçet's disease (BD) was first described in 1937 by Hulusi Behçet, a Turkish dermatologist, as a triad of recurrent aphthous stomatitis, genital aphthae, and relapsing uveitis.1 Although intestinal lesions associated with BD may cause serious complications, such as perforation, and decrease the patient's quality of life, the diagnosis and management of intestinal BD have not been standardized. Empirical therapies have been used anecdotally to treat intestinal BD. However, evidence is accumulating that anti-tumor necrosis factor α (anti-TNF-α) monoclonal antibodies (mAbs) are effective treatments for this indication. In Japan, the anti-TNF-α mAbs, adalimumab (ADA) and infliximab (IFX), are both approved for the treatment of intestinal BD. The introduction of these agents may change our therapeutic strategy and make us reconsider conventional therapies for intestinal BD.
MEDICAL TREATMENT
1. 5-Aminosalicylic Acid
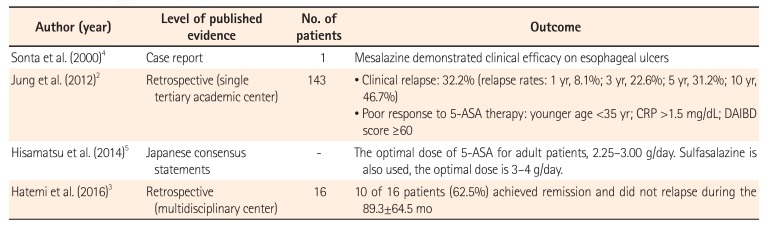
Although there is little clinical evidence for its efficacy, 5-aminosalicylic acid (5-ASA) is used as an empirical therapy for intestinal BD (Table 1). Jung et al.2 retrospectively investigated the long-term clinical outcomes and predictors of clinical relapse in patients with intestinal BD receiving 5-ASA therapy. They found that for 143 patients who received 5-ASA therapy, the cumulative relapse rates at 1, 3, 5, and 10 years after remission were 8.1%, 22.6%, 31.2%, and 46.7%, respectively. In this study, younger age (<35 years), higher CRP level (≥1.5 mg/dL), and higher disease activity index for intestinal Behçet's disease (DAIBD) score (≥60) were associated with a poor response to 5-ASA therapy. Hatemi et al.3 retrospectively reviewed the treatment of 60 BD patients with gastrointestinal lesions. In 16 patients with mild disease, 5-ASA was used as initial treatment. Sonta et al.4 reported an intestinal BD patient in whom 5-ASA was effective for the treatment of esophageal ulcers. These reports suggest that 5-ASA may have clinical efficacy as induction and maintenance therapy for intestinal BD; however, further studies, including placebo-controlled trials, are necessary to confirm this. In their consensus statement, Japanese experts recommended 5-ASA for induction therapy of patients with mild to moderate intestinal BD.5
2. Corticosteroids
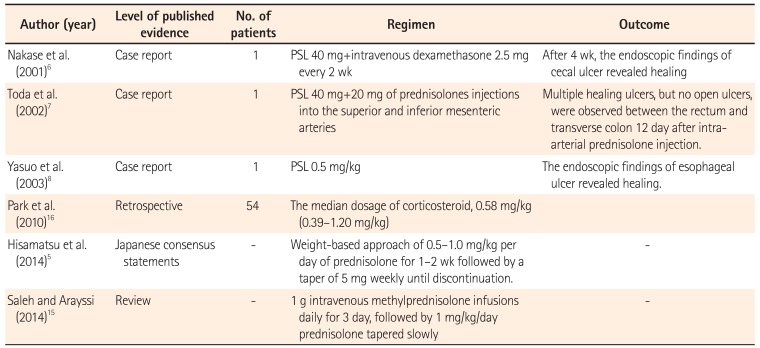
To date, there have been no prospective studies demonstrating the clinical efficacy of corticosteroids in intestinal BD, despite the fact that they have been used empirically for moderate to severe and refractory intestinal BD (Table 2).67891011 The Japanese consensus guideline recommends 0.5 to 1.0 mg/kg/day of prednisolone for 1 to 2 weeks as induction therapy, followed by tapering at 5 mg/wk.51213 In severe cases, an intravenous high dose of prednisolone (1 mg/kg) or methylprednisolone pulse (1 g/day for 3 days) can be used.1415 Park et al.16 reported that clinical remission and response rates to corticosteroid therapy are 46% and 43%, respectively. However, 1 year later, 35.2% of patients who achieved clinical remission showed steroid dependency and 7.4% of patients had undergone surgery. Kimura et al.17 retrospectively reviewed 34 patients with intestinal BD and compared the characteristics of patients treated with corticosteroids and/or 5-ASA (n=8) with those of patients with refractory disease who required additional immunosuppressants, anti-TNF-α mAbs, or surgery (n=12). In the refractory group, more ulcers outside the ileocecal region, more active intestinal bleeding, higher positivity for HLA-B51, higher blood CRP levels, and a higher white blood cell count at onset were observed. In particular, the presence of melena, expression of HLA-B51, or level of CRP >4 mg/dL was identified as predictive factors for refractory BD.
3. Immunomodulators
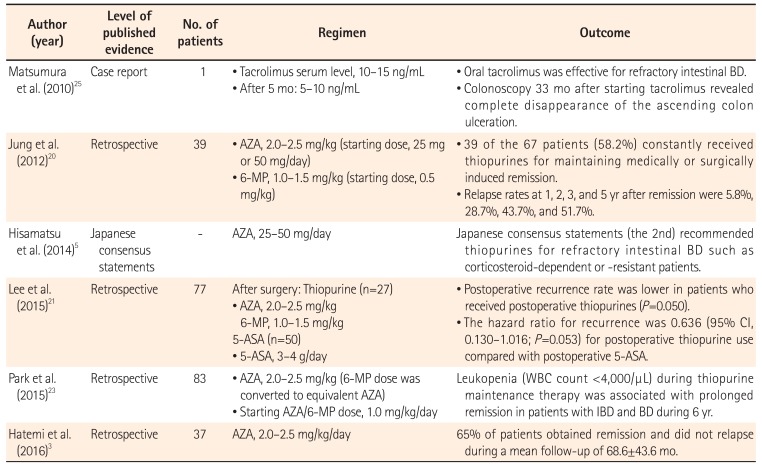
Azathioprine and 6-mercaptopurine are widely used to treat patients with intestinal BD, especially in moderate to severe or refractory disease (Table 3). Jung et al.20 retrospectively reviewed all patients with intestinal BD who received thiopurine therapy. Of a total of 272 patients, 67 (24.6%) received their first course of thiopurine therapy at their center, and 39 of the 67 patients (58.2%) received thiopurines for maintenance of clinical remission. The cumulative relapse rates at 1, 2, 3, and 5 years after remission were 5.8%, 28.7%, 43.7%, and 51.7%, respectively. Japanese consensus guidelines recommend thiopurines for patients with refractory intestinal BD, such as corticosteroid-dependent or corticosteroid-resistant patients.5 Hatemi et al.3 supported azathioprine as a good choice for first-line therapy, because 65% of their patients entered remission and did not relapse during the mean follow-up of nearly 6 years. Lee et al.21 reviewed a total of 77 patients with intestinal BD who received 5-ASA (n=50, 64.9%) or thiopurine (n=27, 35.1%) therapy after surgery. The postoperative recurrence rate was lower in patients who received thiopurines than in patients treated with 5-ASA (P=0.050). The hazard ratio for recurrence was 0.636 (95% CI, 0.130–1.016; P=0.053) for postoperative thiopurine compared with that for 5-ASA. However, the rates of reoperation, readmission, and death were not significantly different between the 5-ASA and thiopurine groups. In contrast, Choi et al.22 reported that the risk of reoperation was lower for patients who received azathioprine than for those who did not. Regarding predictive factors, Park et al.23 reported that leukopenia (white blood cell count, <4,000/µL) during thiopurine therapy was associated with prolonged remission in patients with IBD and BD.
4. Thalidomide
Thalidomide has been identified as an anti-inflammatory and immunomodulatory agent because of its inhibitory effect on TNF-α. Although clinical evidence is lacking, thalidomide and its analog lenalidomide are sometimes used for the management of CD,262728 and there are several studies that report the efficacy of thalidomide in intestinal BD.2930313233 Travis et al.29 reported that thalidomide was used for maintenance therapy in patients treated with IFX. Terrin et al.30 also described a pediatric BD patient with diarrhea who was treated with thalidomide. In a report by Kari et al.,31 5 pediatric BD patients were treated with thalidomide at 1 mg/kg/wk to 1 mg/kg/day, resulting in complete remission in 3 patients and clinical response in 2. Sayarlioglu et al.32 reported a patient who required multiple surgeries due to intestinal perforations and was refractory to intense immunosuppressive therapies, including methylprednisolone and cyclophosphamide. Thalidomide (100 mg/day) was started after the third surgery, and the patient experienced no additional intestinal perforations during the follow-up period of 4 months.
Yasui et al.33 reviewed the cases of 7 patients with juvenile-onset BD with severe, recurrent intestinal involvement. Thalidomide was started at 2 mg/kg per day followed by dose adjustment according to the initial response. All 7 patients showed dramatic improvement in clinical symptoms and they successfully discontinued corticosteroid therapy. Thus, there is evidence to support the clinical efficacy of thalidomide for intestinal BD, especially pediatric BD. Nevertheless, the evidence is still insufficient, and evidence from large cohort and prospective studies is needed.
5. Anti-TNF-α mAbs
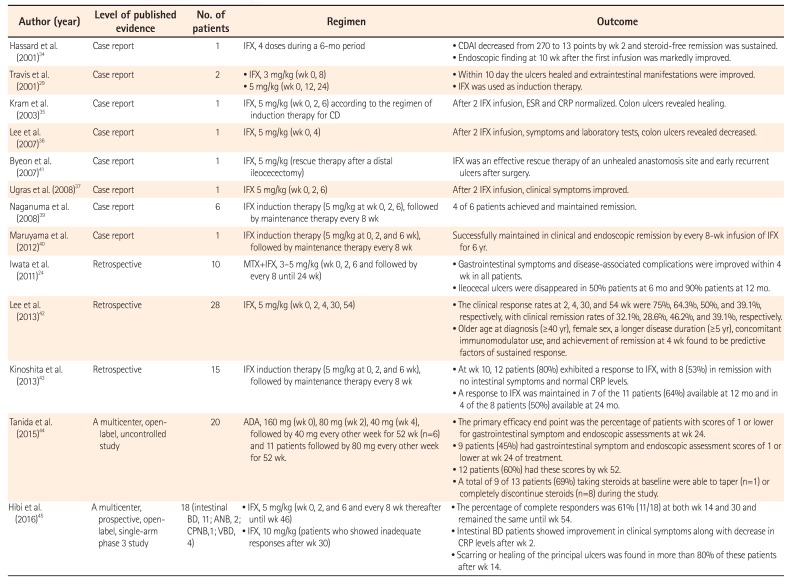
The use of anti-TNF-α mAb therapy for intestinal BD was first reported in 2001 by Hassard et al.34 They treated a patient with steroid-dependent intestinal BD with 4 doses of IFX over a 6-month period. The CDAI score, used as a clinical parameter of disease activity, decreased from 270 points before infusion to 13 points by week 2. With IFX, steroid-free remission was sustained. Endoscopic findings at 10 weeks after the first infusion showed marked improvement of intestinal lesions.34 Travis et al.29 reported the successful treatment of 2 patients having intestinal BD with IFX. Both cases were refractory to corticosteroids and other treatments, including thalidomide and cyclosporine. Within 10 days of IFX administration, the ulcers had healed and extraintestinal manifestations had improved. In these 2 patients, IFX was used as induction therapy, but not as scheduled maintenance therapy. Kram et al.35 described the successful treatment of a patient with 3 infusions of IFX at weeks 0, 2, and 6, according to a regimen of induction therapy for CD.
Since these early reports, evidence of the therapeutic utility of anti-TNF-α mAb in intestinal BD has accumulated (Table 4). Early on, IFX was the anti-TNF-α mAb most frequently used in intestinal BD,3637 with the exception of 1 patient treated with ADA.38 In addition, IFX was used as an episodic treatment or as induction therapy (at weeks 0, 2, and 6),2934353637 but not as a scheduled maintenance therapy. However, after the establishment of a scheduled maintenance regimen of anti-TNF-α mAb for CD (every 8 weeks), there were a number of reports of anti-TNF-α mAbs used for both induction and scheduled maintenance therapy in intestinal BD. Naganuma et al.39 reported on 6 Japanese patients with intestinal BD, all of whom were steroid dependent and refractory to other treatments, who received IFX induction therapy (5 mg/kg at 0, 2, and 6 weeks), followed by maintenance therapy every 8 weeks. Four of the 6 patients achieved and maintained remission with IFX. Iwata et al.24 assessed the short- and long-term efficacy and safety of combination therapy with IFX and methotrexate in 10 patients with refractory intestinal BD. Gastrointestinal symptoms and disease-associated complications improved within 4 weeks in all patients, and ileocecal ulcers had disappeared in 50% (5/10) and 90% (9/10) of patients at 6 and 12 months, respectively. Maruyama et al.40 described a patient with steroid-refractory intestinal BD who was successfully maintained in clinical and endoscopic remission by an infusion of IFX (5 mg/kg) every 8 weeks for 6 years. A retrospective noncontrolled review of the medical records of 28 patients with intestinal BD who received at least one dose of IFX in Korea identified clinical response rates of 75%, 64.3%, 50%, and 39.1%, and clinical remission rates of 32.1%, 28.6%, 46.2%, and 39.1%, at 2, 4, 30, and 54 weeks, respectively, after IFX infusion.42 In another study, 15 patients with active intestinal BD were treated with IFX (5 mg/kg every 8 weeks) at a single center. At week 10, 12 patients (80%) exhibited a response to IFX; 8 (53%) were in remission with no intestinal symptoms and normal CRP levels. A response to IFX was maintained in 7 of the 11 patients (64%) available at 12 months and in 4 of the 8 patients (50%) available at 24 months.43
A prospective clinical trial in Japan was started based on accumulating case reports of the efficacy of anti-TNF-α mAbs in patients with intestinal BD. This multicenter, openlabel, uncontrolled study aimed to evaluate the efficacy and safety of ADA in patients with intestinal BD who were refractory to corticosteroid and/or immunomodulator therapies.44 Twenty patients were administered 160 mg ADA at the start of the study and 80 mg 2 weeks later, followed by 40 mg every other week for 52 weeks. For some patients, the dose was increased to 80 mg every other week. The primary efficacy endpoint was the percentage of patients with a score ≤1 for gastrointestinal symptoms and endoscopic assessments at week 24. This endpoint was reached by 9 patients (45%) at week 24 of treatment, and by 12 patients (60%) by week 52. A total of 9 of 13 patients (69%) taking steroids at baseline were able to taper (n=1) or completely discontinue steroids (n=8) during the study.
Following the clinical trial of ADA, a multicenter, prospective, open-label, single-arm, phase 3 study was performed to determine the efficacy, safety, and pharmacokinetics of IFX in BD patients with serious complications, including gastrointestinal, neurological, or vascular involvement, who had shown poor response or intolerance to conventional therapy.45 IFX was administered at weeks 0, 2, and 6, and then every 8 weeks thereafter until week 46. The dose was increased to 10 IFX/kg in patients who showed inadequate responses to IFX after week 30. The percentage of complete responders (according to predefined criteria depending on the symptoms and results of ileocolonoscopy) at week 30 was defined as the primary endpoint. The percentage of complete responders was 61 (11/18) at weeks 14 and 30 and remained the same until week 54. With IFX, clinical symptoms dramatically improved and CRP levels decreased at week 2. Not only clinical symptoms, but also endoscopic findings rapidly improved. Scarring or healing of the principal ulcers was found in more than 80% of these patients after week 14. Collectively, these case reports and clinical trials provide evidence for the efficacy of anti-TNF-α mAbs in intestinal BD, at least for induction therapy. ADA and IFX efficacy was observed to be rapid by analysis of clinical, serological, and endoscopic endpoints.4445 Although further evidence will be necessary, it is expected that both ADA and IFX will demonstrate long-term maintenance efficacy24404445 and endoscopically evident healing of ulcers.404445
Anti-TNF-α mAbs have not yet been established as a postoperative therapy in patients with intestinal BD who have undergone bowel resection. Byeon et al.41 described a patient with intestinal BD who was successfully treated with IFX as rescue therapy for an unhealed anastomosis site and early recurrent ulcers after surgery.
There is no consensus about the concomitant use of immunomodulators and anti-TNF-α mAbs for intestinal BD, despite anecdotal evidence of its efficacy as induction and maintenance treatment. Even for CD, it remains unresolved whether anti-TNF-α mAbs should be used in combination with immunomodulators.4647484950
6. Mucosal Healing as a Predictive Marker for Long-Term Prognosis
Intestinal BD is a progressive disease that causes dysfunction of the digestive tract and IBD. Postoperative disease recurrence is common, and multiple surgeries are often required in patients with refractory intestinal BD or CD. Since clinical symptoms and the clinical activity index of IBD are often subjective, discrepancies between clinical symptoms and endoscopic findings are often observed. To date, endoscopic findings have been considered the gold standard objective parameter for evaluation of IBD activity. Mucosal healing, defined as endoscopic remission, has become the goal of IBD treatment. Many retrospective studies have indicated that mucosal healing may predict better long-term prognosis, including maintenance of clinical remission, reduced risk of surgery, and reduced risk for the development of colon cancer.51 Although there is currently insufficient evidence, the concept of “mucosal healing” may also be applicable to the management of intestinal BD. Lee et al.52 reported that the discrepancy between the clinical activity index and endoscopic findings is observed not only in IBD but also in intestinal BD. Yim et al.53 retrospectively reviewed the medical records of 80 patients with intestinal BD who underwent colonoscopy within 3 months of clinical remission. At the time of clinical remission, 57 patients (71.3%) had active ulcers and 23 patients (28.7%) achieved mucosal healing. At the follow-up point, 39 patients (68.4%) in the active ulcer group but only 7 (30.4%) in the mucosal healing group experienced recurrence. The cumulative recurrence rate was significantly higher in the active ulcer group than in the mucosal healing group (P<0.001), suggesting that mucosal healing could be a predictive factor for long-term prognosis in intestinal BD. Several case reports and 2 clinical trials (ADA and IFX) have shown that anti-TNF-α mAbs can induce and maintain mucosal healing in intestinal BD patients.404445 Further prospective analyses will be necessary to prove that achievement of mucosal healing improves long-term prognosis in terms of a reduced clinical relapse rate and risk of surgery.
SURGICAL TREATMENT
1. Risk of Surgery and Prognosis
About 3% to 16% of patients with BD have gastrointestinal tract involvement.12 The natural history of intestinal BD has not been clearly delineated and it is difficult to predict which patients will experience a poor clinical course. In a retrospective review of 20 patients, Naganuma et al.54 reported that the presence of ocular and ileal lesions was a risk for surgery. Jung et al.55 evaluated the clinical course of 130 intestinal BD patients during the first 5 years after diagnosis, and found that the majority of patients (74.6%) achieved remission or mild clinical activity at 5 years, whereas 16.2% had multiple relapses or chronic symptoms. Furthermore, the clinical course over the first year after diagnosis influenced the course in subsequent years. Patients in the severe clinical course group were younger, had lower albumin levels, and had higher ESR, CRP levels, and DAIBD scores than patients in the mild clinical course group.
Despite the evident benefits of medical therapy, intestinal BD patients sometimes require surgery and may experience postoperative disease recurrence. Intestinal BD is associated with complications such as intestinal perforation, bleeding, and abscess, and intestinal involvement is therefore a poor prognostic indicator for BD patients. Perforation and massive gastrointestinal bleeding are absolute indications for surgery, and abdominal abscess, fistula, and stricture should be considered as possible indications. Other surgery candidates are intestinal BD patients who are refractory to medical treatment, including corticosteroid and anti-TNF-α mAbs. However, surgery should be carefully considered in these patients because of the risk of postoperative recurrence. Thus, intestinal BD should be considered a progressive disorder, at least in a subpopulation of patients. Chung et al.56 performed a retrospective review of 93 patients with intestinal BD who received medical therapy, and found cumulative recurrence rates of 24.9% at 2 years and 43.0% at 5 years. The presence of gastrointestinal symptoms at the initial presentation was a risk for recurrence. Patients with volcano-type and deep intestinal ulcers, and those who failed to achieve complete remission during the initial treatment, also had a risk of recurrence. Cumulative rates for surgery were 6.7% at 2 years and 15.1% at 5 years. The typical type of ulcer was the only predictive factor for the likelihood of surgery. Moon et al.57 reviewed 129 patients with intestinal BD. Among them, 33 patients had intestinal perforations and all underwent emergent or elective laparotomy. Younger age (≤25 years) at diagnosis, history of prior laparotomy, and volcano-shaped intestinal ulcers were identified as independent risk factors for free bowel perforation in these patients.
One concern about surgical treatment in intestinal BD patients is the risk for postoperative disease recurrence requiring repeat surgery. Iida et al.58 reported that postoperative recurrence of intestinal ulcers was observed in 7 of 9 patients who had undergone a total of 15 operations. Jung et al.59 reported that 42 (58.3%) of 72 Korean patients who had undergone surgery experienced postoperative recurrence, with 22 (30.6%) requiring reoperation. The cumulative 2- and 5-year recurrence rates after surgery were 29.2% and 47.2%, respectively.
2. Postoperative Treatment
To date, a standard postoperative treatment strategy for intestinal BD patients has not been established. The clinical benefit of postoperative thiopurine therapy is controversial. Lee et al.21 reviewed the outcomes of 77 patients with intestinal BD and found lower postoperative recurrence rates in patients who were treated postoperatively with thiopurines, compared with those receiving 5-ASA. However, there were no significant differences in the rates of reoperation, readmission, or death between the 2 groups. In contrast, Choi et al.22 reported that patients who received azathioprine postoperatively showed better clinical courses than those who did not. Thalidomide was also used as a postoperative therapy in a patient who required multiple surgeries.32 To date, there are no reports reviewing the efficacy of postoperative anti-TNF-α mAbs therapy in intestinal BD patients.
FUTURE PERSPECTIVES
Accumulating clinical evidence supports the efficacy of anti-TNF-α mAbs for intestinal BD and may change the therapeutic strategy for this disease. Most importantly, the natural history of refractory patients and their risk factors should be identified. The importance of endoscopic remission for monitoring disease activity has not been fully accepted in the management of intestinal BD, as it has for IBD. In addition, further clinical studies are necessary to evaluate immunomodulators and anti-TNF-α mAbs as maintenance therapy for intestinal BD. Postoperative management of intestinal BD also needs to be standardized, both to decrease the risk of repeat surgery and to improve the quality of life for postoperative patients.
 XML Download
XML Download