

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Thromboembolism in acute coronary syndrome or atrial fibrillation is largely prevented by anti-thrombotic agents12. However, bleeding complications related to these agents after minor oral surgery is of concern to dentists for dental management of these patients. Risks and benefits of the anti-thrombotic agents must be weighed before initiating dental procedures, which should be established as treatment guidelines. The purpose of this paper is to optimize the management of dental patients on anti-thrombotic medication via standardized treatment protocols. The target readership of the paper is undergraduate and postgraduate dental students, general dental practitioners, trainees and residents of oral and maxillofacial surgery, and oral and maxillofacial surgeons.
II. Background
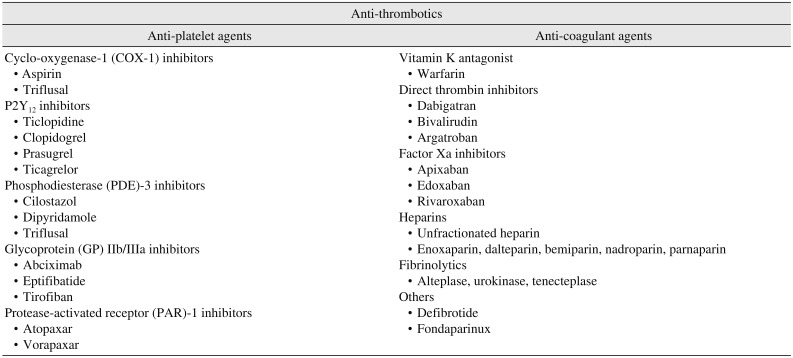
Hemostasis occurs as a result of the interaction of the components of Virchow's triad, namely endothelial cells, blood composition and vascular flow. Interplay of these three factors determines the chance of thrombotic accident. Arterial thrombosis is related to platelet-rich white clots, whereas venous thrombosis is related to fibrin-rich red clots3. Anti-thrombotic agents are classified into two categories, anti-platelets and anti-coagulants, which are listed in Table 14. While anti-platelet agents inhibit platelet aggregation, anti-coagulant agents block the coagulation cascade after platelet aggregation. Anti-platelet agents are useful for the prevention and treatment of platelet-rich white clot formation, whereas anti-coagulant agents prevent and treat venous thromboembolism. Currently popular anti-thrombotic agents in Korea will be discussed briefly.
1. Anti-platelet agents
1) Aspirin (Astrix)
Aspirin is an anti-inflammatory drug that inhibits the cyclooxygenase pathway of arachidonic acid, which is mobilized in the inner cellular membrane5. In inhibiting this pathway, aspirin also inhibits the production of thromboxane, making it a standard for treatment of ischemic heart diseases. It can be used as a single load or used in combination with clopidogrel in dual antiplatelet therapy (DAPT)67. There are more thromboembolic complications after discontinuation when aspirin is used for secondary prevention than when used for primary prevention89, which necessitates careful consideration of aspirin discontinuation, especially when it is used in secondary prevention of thromboembolic complication.
2) Clopidogrel (Plavix)
In contrast to aspirin, which impairs thromboxane-mediated platelet activation, clopidogrel is a purinergic receptor antagonist that inhibits binding of P2Y12 receptors on the platelet surface with adenosine diphosphate (ADP)10. It can be administered at a rate of 75 mg once a day for primary prevention. In cases of acute coronary syndrome, the initial loading dose is 300 mg, followed by a daily maintenance dose of 75 mg. In cases of secondary prevention, it is more effective in preventing thromboembolism when used concomitant with aspirin (DAPT).
3) New anti-platelet agents
(1) Prasugrel (Effient)/ticagrelor (Brilinta)
Clopidogrel is a prodrug whose bioactive form is created through enzymatic cleavage in the liver. Metabolism of clopidogrel through hepatic enzyme CYP2C19 into its active form is a time-consuming process, and clinical efficacy of clopidogrel is largely dependent on inter-individual differences caused by genetic variability of expression of the enzyme CYP2C1911. Prasugrel is the same type of prodrug as clopidogrel, but is less subject to genetic variability and rapidly becomes biologically active because of differences in the metabolic pathways1213. Ticagrelor is different from clopidogrel or prasugrel, which are thienopyridines; it has a reversible inhibitory action against P2Y12 receptor. Ticagrelor exerts its action via binding to the P2Y12 receptor in a manner different from ADP, resulting in an allosteric antagonist14.
(2) Vorapaxar (Zontivity)
Thrombin is a serine protease that exhibits the most potent platelet activation at subnanomolar concentrations, in contrast to ADP, which requires micromolar concentration to exhibit its action1516. Thrombin action on platelets is mediated via platelet protease-activated receptors (PARs). Vorapaxar is a reversible PAR-1 inhibitor that directly inhibits thrombin action. Large phase III trials resulted in clinical effect for reducing atherothrombotic event in addition to current standard anti-platelet therapy17. However, with clinical data still being accumulated, a cardiology consult is recommended before dental procedures.
2. Anti-coagulants
1) Warfarin (Coumadin)
Warfarin is used where blood flow is relatively static, making its use effective for treatment of deep vein thrombosis or pulmonary embolism and for prevention of stroke in patients with atrial fibrillation, valvular heart disease or artificial heart valves18. Its effects are monitored using the prothrombin time/international normalized ratio (PT/INR). It is administered orally, with few days required for its full pharmacologic action, which lasts for about five days.
2) NOACs
The term NOACs refers to novel (new) oral anticoagulants, also called “non-vitamin K antagonist oral anticoagulants” and “directly acting oral anticoagulants” (DOAC). They exhibit rapid onset time and prompt withdrawal of the anticoagulation effect when stopped because of their rapid action and short half-lives, respectively19202122. Their predictable anti-coagulative activity decreases the need for monitoring relative to that required during warfarin therapy. Despite relatively little data, they are known to have few drug interactions and are less affected by diet23.
(1) Dabigatran (Pradaxa)
Dabigatran is an oral preparation directly inhibiting thrombin. It is currently the only NOAC that has an antidote, idarucizumab, which reverses the anti-coagulative action of dabigatran within minutes24. The most reported adverse reaction of this drug is gastrointestinal (GI) upset25. It is contraindicated in patients with mechanical prosthetic heart valves to avoid thromboembolic events26.
(2) Rivaroxaban (Xarelto)
Rivaroxaban is the first direct factor Xa inhibitor of oral preparation that belongs to the same type as apixaban (Eliquis) and edoxaban (Savaysa, Lixiana). It inhibits factor X competitively and is dose-dependent in its efficacy. With fewer complications than warfarin, the most known complication with rivaroxaban is GI bleeding. Rivaroxaban, along with apixaban and edoxaban, exhibited superior effectiveness with equal or reduced risk of bleeding compared to warfarin27.
III. Bleeding Risk Assessment
1. Bleeding tendency according to procedural differences
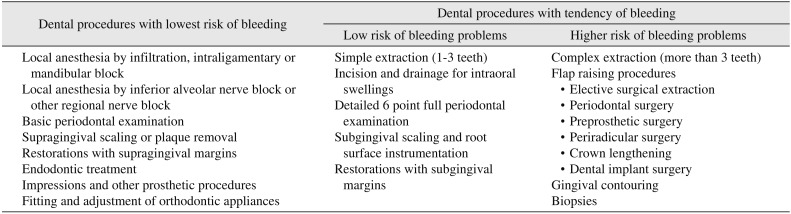
Significant bleeding after dental procedures is relatively rare in patients of continued anti-coagulant therapy. However, any bleeding complications after minor oral surgery are of concern to dentists. Bleeding complication means prolonged or excessive bleeding or bleeding not controlled by initial hemostasis. Relevant dental procedures and their respective postoperative bleeding risks are listed in Table 219. Those procedures that cause little bleeding are straightforward in patients on anti-thrombotic agents with use of standard practices to avoid bleeding. Dental procedures that are likely to cause bleeding are categorized as either low-risk or high-risk procedures. Careful patient selection according to this criteria helps prevent bleeding complications.
2. Bleeding tendency related to patients' medical conditions
In general, the evidence-based guidelines published by American Academy of Neurology recommend that anti-thrombotic medication be continued without change in patients with ischemic cerebrovascular disease28. Individual patients' characteristics are an important consideration for assessment of risk and benefit. Patients with ischemic heart disease who did not undergo coronary stent surgery belong to the low-risk group, whereas patients with prosthetic heart valve concomitant with atrial fibrillation are considered high-risk. Likewise, those with mechanical prosthetic valve are of consideration because they are not candidates for NOACs26. Concerned patients' medical conditions that are prone to develop thrombo-embolism are listed up in Table 329.
3. Other considerations
Many clinical trials have revealed similar or lower incidence of major bleeding events among patients taking NOACs than among those taking warfarin303132. However, clinical experience indicates that that clots typically form quickly, but also become dislodged easily in patients on anti-coagulants. Meanwhile, anti-platelet medication may lead to delayed clotting after invasive procedures, but once formed, clots tend to be more stable in those patients on anti-platelets than in patients on anti-coagulant medication. Additional risk factors for postoperative bleeding are possible if the patient has decreased renal function, liver function, or bone marrow disorders33. Some herbal and complementary medicines such as garlic may be related to bleeding risk. Recently, an ultra-high risk group was added to the classification of patients on anti-thrombotic agents by the Asian Pacific Association of Gastroenterology (APAGE) and the Asian Pacific Society for Digestive Endoscopy (APSDE)34, which should be conferred by other guidelines including our own.
IV. Bleeding Risk Management
General dental management principles for patients on anti-thrombotic agents recommend following standard procedures to avoid causing bleeding. If the anti-thrombotic medication is not prescribed as a life-long medication, dental treatment may be delayed until after discontinuation of the medication. For patients with prosthetic metal heart valves or coronary stents, direct written instructions from the cardiologist are required to alter their anti-thrombotic medications. Analgesic medications such as aspirin, ibuprofen and diclofenac can exacerbate the bleeding risk of the patient and should be prescribed carefully.
The most useful hemostasis is local mechanical arrest, such as packing of open sockets with hemostatic material and suture35. There is no reason to interrupt anti-thrombotic medication if the patient is taking aspirin alone, because there is no evidence of higher bleeding risk in these patients than in nonantithrombotic patients. Scheduling elective procedures early in the day and week is recommended for patients on anti-thrombotic agents to allow time for bleeding control, in case of bleeding episodes.
1. Dental management of patients on anti-platelet agents
With no suitable test for measuring anti-platelet effects causing bleeding, it is common belief that dual antiplatelet medication tends to prolong bleeding compared to aspirin alone. However, it is recommended that dental management be given without altering antiplatelet medication for patients on aspirin alone or on DAPT28363738. Patients who undergo a coronary artery stent surgery must keep their anti-platelet prescription for up to 12 months.
If the patient is on aspirin alone, it is recommended that the initial treatment site be limited, that is, extract only a single tooth or limit the subgingival scaling to three teeth, so that bleeding can be assessed before further procedures. For procedures with anticipated higher bleeding complications, staged treatment with active engagement of local hemostatic measures such as suturing and packing should be considered.
Currently the most commonly used dual antiplatelet medication is the combination of aspirin with clopidogrel. In such a case hemostasis may be delayed up to an hour, which will justify limitation of the initial treatment site, e.g., a single extraction or limitation of the subgingival scaling to three teeth before further procedures. For procedures with a higher risk of postoperative bleeding, staged treatments over separate visits and active engagement of local hemostatic measures is recommended.
There are occasions that require complex anti-thrombotic therapy. Patients with atrial fibrillation often have coexisting vascular disease such as ischemic heart disease. In such a coexisting diagnosis, combined medication is required with continued oral anticoagulation and platelet inhibitor therapy39. In rare cases of triple drug combinations or other combinations such as aspirin with warfarin or clopidogrel with warfarin, the risk of postoperative bleeding is higher, which necessitates medical consultation with the prescribing physician.
2. Dental management of patients on warfarin or other vitamin K antagonists
The key recommendation for a patient on warfarin is that there is no alteration of the vitamin K antagonist medication with an INR below 428384041. If the patient's INR is stable, INR checking within 72 hours before the dental procedure is acceptable, whereas INR should be checked no more than 24 hours before when INR is unstable. It should be kept in mind that stable INR means INR measurements had not been above 4 in the last two months42. If the INR is over 4, the dental procedure should be delayed until correction by anti-coagulation management by medical personnel. Additionally, limiting the initial treatment site or staging treatment over separate visits for procedures with higher risk of bleeding should be considered.
3. Dental management of patients on NOACs
The NOACs currently available in clinical use are either too sensitive or too insensitive to PT/INR test43. However, monitoring of NOACs is less critical than that of warfarin because these drugs are more stable in anticoagulation44. NOACs have a rapid onset time and short half-lives compared to warfarin202122, which makes their anti-coagulation activity minimized and suboptimal. In this respect, dental management of patients on NOACs is more predictable than that of those on warfarin. Although there have been few NOACs with available antidotes (with the exception of idarucizumab for dabigatran24), the quickness of the anti-coagulation effect of NOACs necessitates less monitoring.
Although there is little published research on the bleeding risks concerning dental procedures for patients on NOACs, key recommendations fall into two categories. Patients who are expected to have dental procedures with a low risk of bleeding are recommended not to alter the anti-coagulant medication. Patient appointments are recommended early in the morning in spite of the peak concentration of drugs, because the bleeding complication, should it occur, could be managed adequately during surgery hours. Limitation of the initial treatment site and active local hemostasis follows the principles described above.
Patients on NOAC who have higher-risk procedures with respect to postoperative bleeding are recommended to skip the morning dose on the day of the dental appointment. If the NOAC prescription is once a day in the evening, patients should not miss the evening medication the night before the dental appointment. Early appointments are recommended to allow time to cope with possible unexpected bleeding complications. Staged treatment over separate visits is also a consideration for such patients. Consideration of active local hemostasis is the same as above. Detailed medication counseling concerning when to restart medication is as follows:
1) Rivaroxaban (once a day): Missed morning dose is followed by the next morning dose after normal dental procedure without any bleeding complication. For patients with evening dose, usual evening dose on the day of early dental procedure is accepted only when four hours of hemostasis is confirmed.
2) Dabigatran and apixaban (twice a day): For those who have missed morning dose, usual evening dose is accepted as long as four hours of hemostasis is confirmed.
3) No missing of subsequent doses is allowed unless an absolute emergency of bleeding.
In rare occasions of emergency situations in patients who have already taken a morning dose, it is advised that higher risk procedures be delayed until later in the day to allow levels of anti-coagulation to decrease.
4. Dental management of patients on injectable anti-coagulant agents
Although limited, patients with parenterally administered low molecular weight heparin (LMWH) may still be encountered in the dental office. These patients include some pregnant woman and patients diagnosed as venous thrombosis that already have cancer. Dalteparin and enoxaparin are available drugs that could administered once daily or twice a day4546. For patients using these drugs, medical consultation is necessary prior to dental procedures because there is no direct clinical evidence concerning dental treatment. Patients with chronic renal impairment may have kidney dialysis, during which patients are given heparinized dialysis solution. Dental procedures must be delayed until the following day.
5. Drug interactions between anti-thrombotic agents and other medications
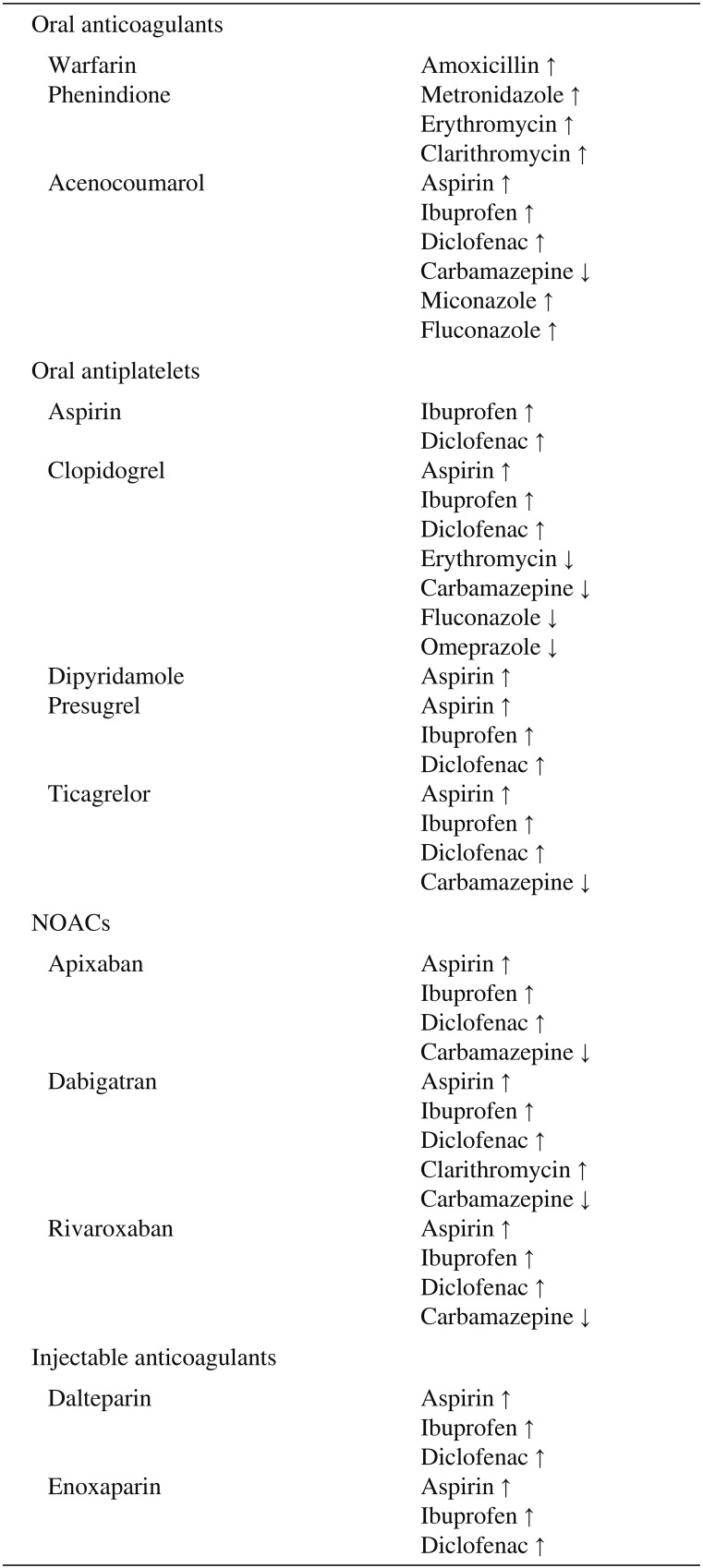
Many drugs prescribed by dentists, such as antibiotics or analgesics, could show drug interaction. Drugs that could have possible interactions with anti-platelet agents or anti-coagulant agents are listed in Table 419. Drugs known to increase the bleeding tendency are indicated with an up arrow(↑). Drugs that could decrease antiplatelet or anticoagulant potential, which will increase the patient's thromboembolic risk, are indicated with a down arrow (↓).
V. Epilogue
The number of geriatric patients seeking dental service is ever rising because of increased life expectancy in conjunction with increased chronic medical conditions. Patients on anti-thrombotic medication fall into this category; treatment guidelines of such patients were described in this review. The consensus meeting on anti-thrombotic agents held on Mar 24, 2018 at Seoul National University Dental Hospital by the Korean Association of Oral and Maxillofacial Surgeons justifies a future consensus paper on dental management of patients on anti-thrombotic medication. Dedicated to future treatment guideline, the author hopes this review will bridge the gap between the current medical environment and that of the near future presenting an official consensus on dental management of patients on anti-thrombotic medication.

 XML Download
XML Download