

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
POEMS syndrome is a rare paraneoplastic syndrome associated with an underlying plasma cell disorder [1]. The acronym POEMS refers to frequently occurring features of the syndrome: polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, and skin changes [2, 3, 4]. Other important clinical features include papilledema, extravascular volume overload, elevated vascular endothelial growth factor (VEGF) levels, pulmonary hypertension, platelet dysfunction, a predisposition towards venous thrombosis, as well as multifocal bone lesions and/or diffuse bone marrow plasma cell infiltration [4]. Neuropathy, such as neuropathic pain or hyperesthesia, is the most predominant characteristic of POEMS syndrome; it afflicts virtually every POEMS patient and severely impairs quality of life [5, 6, 7, 8, 9].
The treatment for POEMS syndrome should involve elimination of the plasma cell clone. In the case of localized plasmacytomas, this may be achieved with local therapy; however, in patients with disseminated disease, systemic treatment is required. Owing to its rarity, there have been no randomized controlled trials of treatment for POEMS syndrome. Several single-center retrospective studies show that high-dose melphalan therapy followed by autologous stem cell transplantation (ASCT) can be an effective treatment for progressive POEMS syndrome. However, very few publications report clinical outcomes in patients with advanced POEMS syndrome and poor performance. Furthermore, most previous studies of ASCT for POEMS syndrome have focused mainly on hematologic response and survival. Hence, the aim of the current study was to summarize our experience using ASCT to treat patients with severe POEMS syndrome, focusing on changes in performance status, neuropathy, and hematologic outcome.
MATERIALS AND METHODS
Study subjects
This study was a retrospective evaluation of 9 advanced POEMS syndrome patients, who underwent high-dose melphalan therapy followed by ASCT from 2004 to 2011 at Asan Medical Center in Seoul, Korea. All 9 patients fulfilled the criteria for diagnosis of POEMS syndrome proposed by Dispenzieri [5]. The diagnosis requires the presence of both major criteria (polyneuropathy and monoclonal plasma proliferative disorder) and at least one minor criterion (bone lesion, Castleman's disease, organomegaly, edema, endocrinopathy, skin changes, and papilledema). The institutional review board of Asan Medical Center approved this study (IRB No.2013-0863) and waived the requirement for informed consent.
Stem cell collection and transplantation
Peripheral blood stem cells were collected from 8 of the 9 patients after mobilization with cyclophosphamide (4 g/m2) and growth factors [10, 11]. Patient number 4 was excluded because of thrombocytopenia. High-dose melphalan (200 mg/m2) was used as the conditioning regimen. All patients received standard supportive care, including prophylactic antibiotics during ASCT [12].
Response assessment
Hematologic responses were defined according to the International Myeloma Working Group criteria [13]. Evaluation of performance and neuropathy were based on detailed medical examinations by neurologists and/or oncologists. After ASCT, the general performance status of all patients was evaluated and monitored according to the Eastern Cooperative Oncology Group (ECOG) performance status scoring system. The following were used to evaluate clinical response: detailed history and physical examination by oncologists and neurologists, and patient-reported outcomes on activities of daily life. Elaborate chart reviews were conducted, including chest x-ray, computed tomography (CT), and echocardiography results, and medications prescribed, particularly for peripheral neuropathy or its symptoms. A nerve conduction velocity test was conducted and repeated whenever peripheral neuropathy developed or worsened before and after ASCT.
RESULTS
Patient characteristics
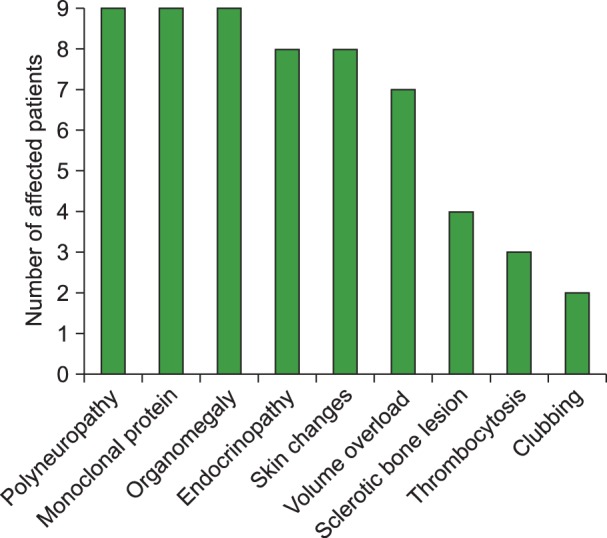
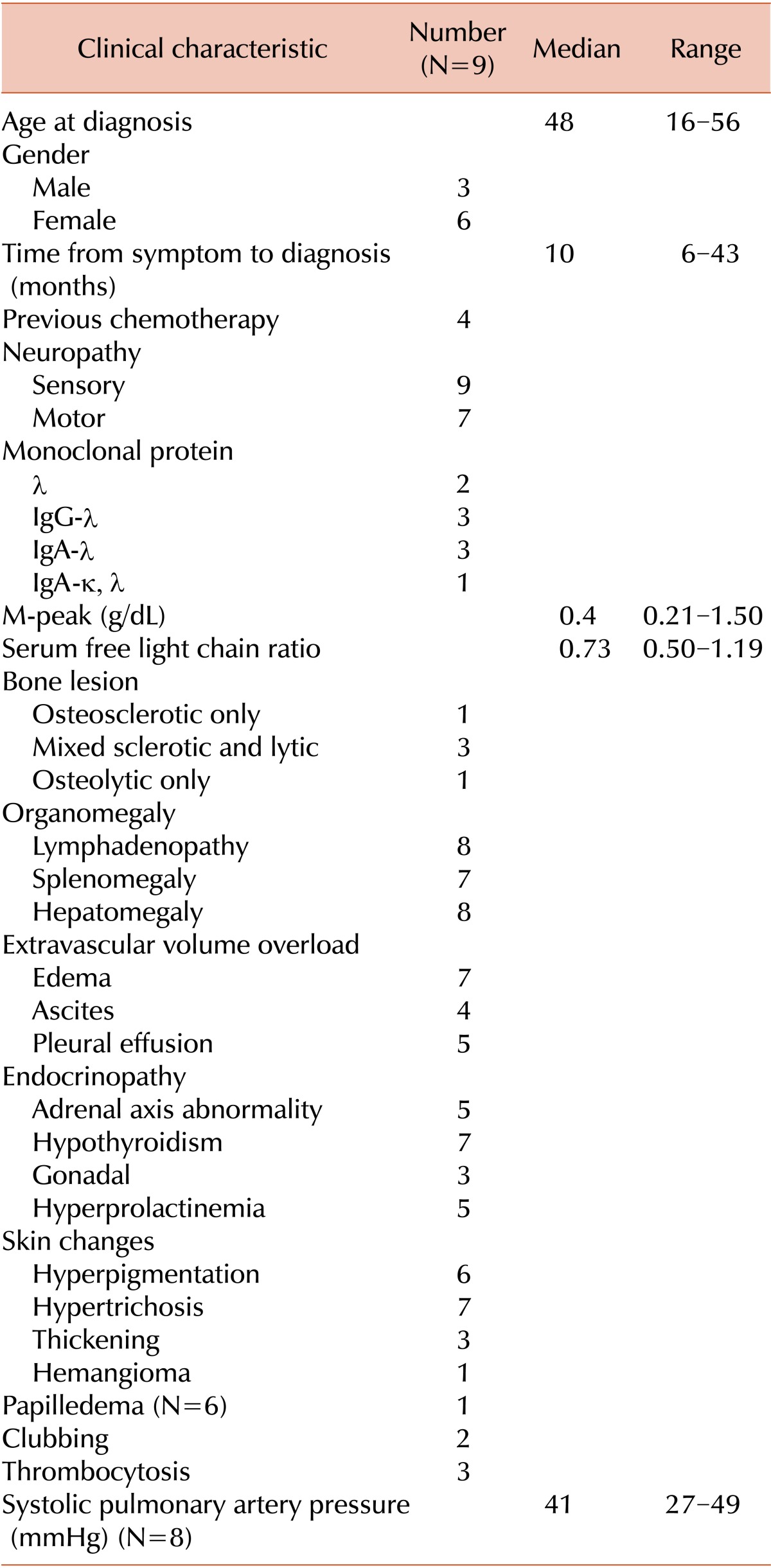
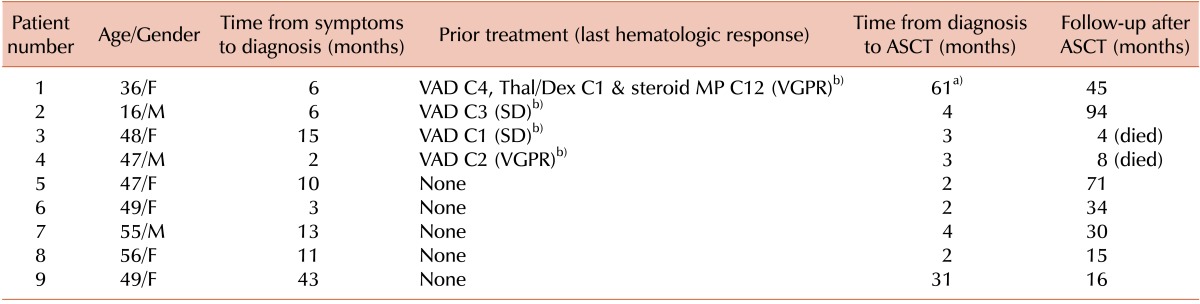
Demographic and clinical features are summarized in Table 1 and Fig. 1. Median age at diagnosis was 48 years (range, 16-56 years). All 9 patients had polyneuropathy, monoclonal plasma cell disorder and organomegaly; 8 of them showed endocrinopathy (abnormality of pituitary, adrenal, thyroid, or gonadal function) and skin changes; none had Castleman's disease. Extravascular volume overload (e.g., peripheral edema, pleural effusion, or pericardial effusion) was found in 7 patients. As shown in Table 2, 4 patients had a history of prior chemotherapy with vincristine, adriamycin, and dexamethasone (VAD) with a median of 3 cycles (range, 1-4 cycles). Of the 4, 2 had a very good partial response to chemotherapy, and 2 had stable disease; however, pre-ASCT chemotherapy was discontinued in all 4 patients because of neurotoxicity. The 5 patients with newly diagnosed POEMS syndrome underwent high-dose melphalan chemotherapy followed by ASCT as first-line treatment without prior chemotherapy.
Hematologic response after ASCT
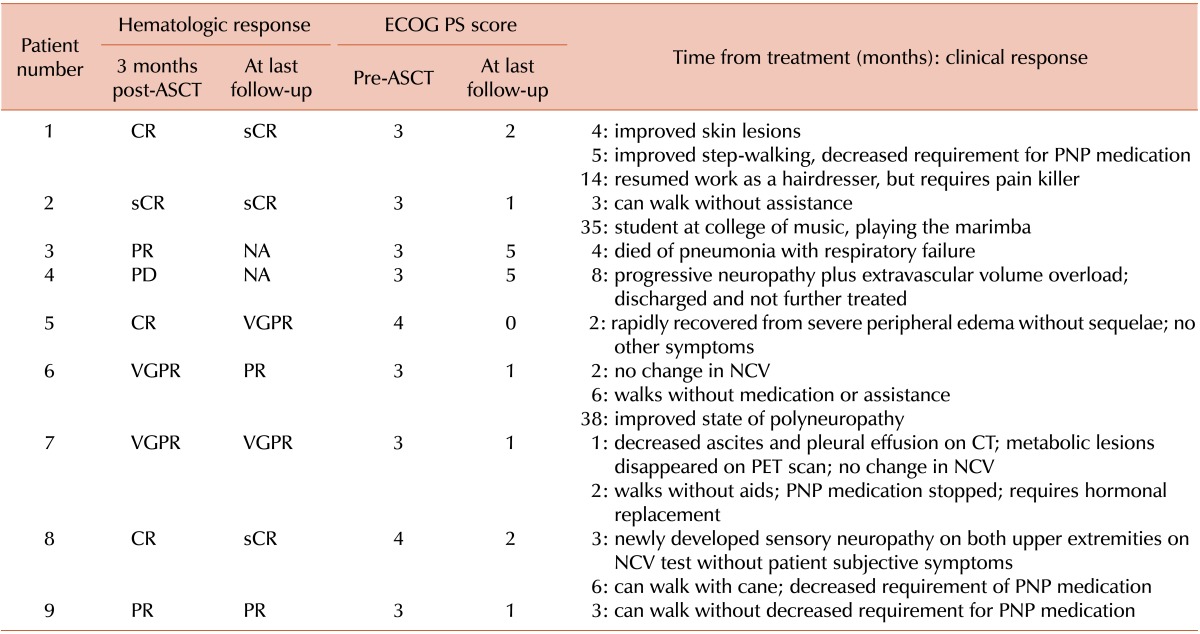
Initial hematologic responses were observed in all 9 patients around 3 months after ASCT, including 3 complete responses (CR) and 1 stringent CR (sCR). Two patients with an initial CR achieved a sCR at 3 months post-ASCT and 9 months post-ASCT (patient numbers 8 and 1, respectively). There were no cases of hematologic relapse during the follow-up period. All survivors showed more than a partial hematologic response through the last follow-up.
Survival
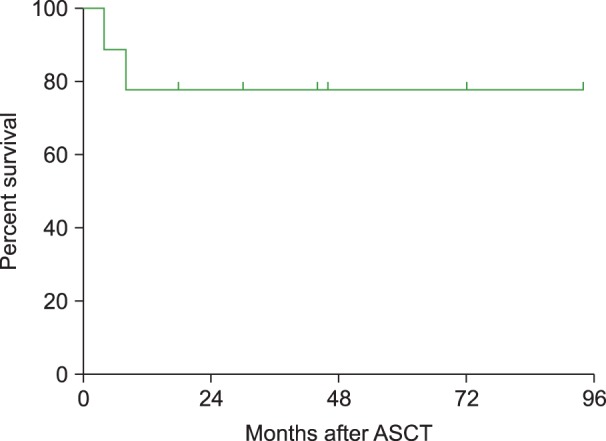
After a median follow-up of 44 months after ASCT (range, 8-94 months), 7 patients were still alive with a 3-year overall survival rate of 77.8% (Fig. 2). One patient died of progressive extravascular overload resulting in intractable pulmonary edema and progressive neuropathy related to POEMS at 8 months after ASCT (patient number 4). Another patient died of pneumonia with respiratory failure despite a hematologic response at 4 months after ASCT (patient number 3) (Table 3).
Details of stem cell collection and transplantation
As shown in Table 2, the median time from symptoms to diagnosis was 10 months (range, 6-43 months), and the median time from diagnosis to ASCT was 3 months (range, 2-61 months). The median number of peripheral blood stem cell mobilizations was 2 (range, 1-5). The median number of CD34-positive hematopoietic stem cells collected was 17.7×106 cells/kg (range, 4.26-66.40×106 cells/kg), and the median number of CD34-positive cells infused was 17.7×106 cells/kg (range, 4.14-48.30×106 cells/kg). The median time for neutrophil recovery to greater than or equal to 500/µL was 10 days (range, 9-13), and median time for platelet recovery to greater than or equal to 50,000/µL was 17 days (range, 13-194). Median duration of hospitalization was 38 days (range, 18-124), and there were no adverse events during stem cell harvest.
One patient experienced the following complications at day 9 post-ASCT: engraftment syndrome with fever, erythrodermatous skin rash on both hands, and mild pulmonary congestion (patient number 8). Patient number 8 recovered within 3 days without corticosteroid treatment. None of the patients suffered from severe transplantation-related complications (including treatment-related mortality).
Change of performance status and neuropathy
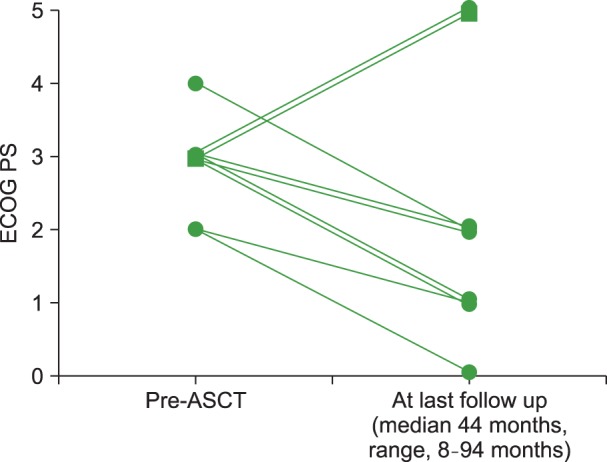
Fig. 3 and Table 3 summarize patient-reported outcomes on activities of daily life as well as the changes in ECOG performance status after ASCT. General performance of all patients at diagnosis was very poor, mainly due to rapidly progressive peripheral neuropathy and extravascular volume overload (peripheral edema, pleural effusion, or ascites). ECOG performance scores were 3 or 4 in all patients before ASCT. After ASCT, ECOG performance scores had improved in all survivors to between 0 and 2 at last follow-up. None of the patients showed deterioration of performance status throughout the follow-up period.
A nerve conduction velocity test was performed on 2 patients prior to and after ASCT. One patient (patient number 6) had no change in nerve conduction velocity at 2 months post-ASCT, but showed improvement when tested at 38 months post-ASCT. The other patient (patient number 8) showed no change in nerve conduction velocity 3 months after ASCT. Although a follow-up nerve conduction velocity test was not performed in patient number 8, the patient needed less medication for neuropathy and could walk with a cane 6 months after ASCT. Daily activity and skin color changes were improved in all patients throughout follow-up. However, there was some discrepancy between improvement in performance or subjective symptoms and changes in peripheral edema or pulmonary edema (Table 3).
DISCUSSION
The efficacy of ASCT in the treatment of advanced POEMS syndrome has been suggested by several studies. In the current study, 9 patients with very poor performance underwent ASCT and 8 of them achieved a hematologic response, with 4 of the 8 being complete responses.
Since 2001, several case reports and case series have been published showing that ASCT can be an effective treatment for POEMS syndrome. Recently, long-term clinical outcomes have been reported for patients with POEMS syndrome after ASCT [13]. However, few studies have included patients with poor performance status. In one study of 8 patients with POEMS syndrome undergoing ASCT that included just 1 patient with an ECOG performance status >2, the reported overall response rate was 87.5%, with 100% improvement in performance status, and no cases of treatment-related mortality or engraftment syndrome [14]. In another study, only 20% of the 59 patients had an ECOG performance status of 3 [13].
Appropriate patient selection is an important issue regarding the risk-benefit ratio associated with ASCT; however, no selection criteria for patients with newly diagnosed POEMS syndrome have been applied thus far. Li and Zhou [15] recently recommended the following exclusion criteria for ASCT: age >65 years, abnormal renal function (serum creatinine >1.326 mg/dL), severe pulmonary hypertension (systolic pulmonary arterial pressure >70 mm Hg), capillary leak syndrome (hypotension and/or refractory ascites), and active infection.
A total of 10 patients have been diagnosed as having POEMS syndrome in our center during the study period. All patients had very poor performance status (ECOG score 3 or 4) at diagnosis. Among them, 9 patients were treated with ASCT during the study period. Seven of the 9 patients had extravascular volume overload (peripheral edema, ascites, or pleural effusion) that seemed to be closely associated with peripheral neuropathy. According to the exclusion criteria by Li and Zhou [15], 7 patients should not have been treated with ASCT because of their abnormal renal function or capillary leak syndrome. Despite the poor performance status of patients in our study, there was no treatment-related mortality after ASCT, and all survivors showed improvement in performance status and neuropathy.
The reported risk of morbidity and complications associated with ASCT for POEMS syndrome have changed over the past decade [15]. In one study, 1 of 30 patients died from treatment-related toxicity, and approximately 50% of patients developed engraftment syndrome. Among those with engraftment syndrome, 10% required temporary dialysis, and 17% required intubation [16]. In 2012, a long-term study of ASCT in 59 patients (median follow-up=45 months) reported clinical responses in 92% of patients and 3 deaths [13]. In our study, 2 patients died during follow-up: 1 died of disease progression despite ASCT; the other died of pneumonia 4 months after ASCT. There was only one case of engraftment syndrome after ASCT. None of the patients suffered from severe transplantation-related complications or treatment-related mortality. Five patients (55.5%) did experience osteosclerotic lesions in this study. If the patients underwent additional positron emission tomography (PET) scans, we might have found more sclerotic lesions.
There is no consensus about optimal dose of melphalan; however, an ASCT regimen of melphalan 200 mg/m2 has been widely applied [17]. The conditioning chemotherapy for all 9 POEMS patients in our study was melphalan 200 mg/m2. In the previously mentioned study of ASCT in 59 POEMS patients [13], 41 patients received melphalan 200 mg/m2, 17 received melphalan 140 mg/m2, and there were only 2 cases of therapy-related myelodysplastic syndrome. Further study is needed regarding the optimal dose of melphalan.
With respect to clinical response, there are several single-center studies showing that high-dose melphalan therapy with subsequent ASCT can effectively control neuropathy in patients with progressive POEMS syndrome [1, 16, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27]. In a number of case series, each containing approximately 100 patients, all patients achieved at least some neurologic improvement [16, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28]. A 100% neurologic response was reported in 9 patients treated in Japan; the neurologic improvements were observed 1 to 3 months after treatment [29]. Another study investigated neurologic improvement in 5 patients after their second round of high-dose ASCT therapy using both neurological examination and patients' subjective assessment of their neurological skills in daily life [17]. However, there are few reports focused on improvement of performance and clinical response from Asian centers. In the current study, we were able to assess ECOG performance score before and after ASCT in all patients. In addition, clinical response was evaluated for each patient by detailed history taking, physical and neurologic examination throughout the study period. In our results, all survivors showed improvement in ECOG performance score from 3 or 4 to between 0 and 2. However, clinical improvement was not apparent until at least 6 months after ASCT (Table 3; Fig. 3). Given the hematologic response and clinical benefit of ASCT, early treatment with ASCT might be considered for patients with poor performance status, especially for those with extravascular volume overload or capillary leakage syndrome.
Limitations in our study include its retrospective design, small sample size, and inadequate evaluation of serum vascular endothelial growth factor (VEGF). Since 2011, VEGF has become one of the major criteria in the revised POEMS criteria, because VEGF is highly correlated with disease activity [1]. Moreover, there was a single domestic center study with 3 POEMS syndrome patients, which showed reduction of serum VEGF levels in all patients after bortezomib followed by ASCT [30]. Unfortunately, VEGF levels and whole body PET scans were not fully evaluated for patients in this study.
Nevertheless, the clinical benefits observed in this study (improvement in performance status and quality of life, as well as the hematologic response and prolonged survival) suggest that high-dose melphalan followed by ASCT is a valid treatment option even for patients with severe POEMS syndrome.
 XML Download
XML Download