

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Fixed drug eruption (FDE) is characterized by the site-specific recurrence of dusky-red to brownish macules or patches that recur with re-administration of the causative drug1. Although FDE usually presents as a solitary lesion, the lesions can be generalized in rare instances. Although cephalosporins are some of the widely prescribed antibiotics worldwide, FDE due to cephalosporins is rarely reported. Here, we report a case of generalized FDE due to cefaclor confirmed by rechallenge.
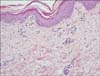
A 64-year-old man presented with generalized brownish patches (Fig. 1A). He had been diagnosed with macular degeneration approximately 2 months earlier, and received 3 injections of bevacizumab. After each injection, he took cefaclor, loxoprofen, and streptokinase/streptodornase at 4-week intervals to reduce pain and prevent secondary infection. Erythematous patches developed 6 hours after he took the oral medicines for the first time. The skin lesions resolved spontaneously, leaving hyperpigmentation. Whenever he took the medicines, new erythematous patches developed and previous hyperpigmented patches darkened. Skin biopsy results were concordant with a clinical diagnosis of FDE (Fig. 2). We explained to him the probable diagnosis, causative drugs, and methods for definite diagnosis. After 3 months, he volunteered to take the 3 abovementioned drugs to identify the causative drug. After he took cefaclor, existing skin lesions became reddish and new lesions developed within 24 hours (Fig. 1B). No skin lesions developed after taking the other drugs. Considering this and his clinical history, he was diagnosed with cefaclor-induced generalized FDE. No skin lesions developed after cefaclor was changed to ofloxacin. However, patch tests performed 8 months later on normal and hyperpigmented areas with 10%, 20%, and 30% pet. cefaclor powder were negative on days 2 and 4.
Cefaclor is a second-generation cephalosporin. Adverse cutaneous drug reactions due to cephalosporin generally cause a morbiliform rash but rarely lead to FDE. There are several tests for identifying the causative drug, including the patch test, prick test, and intradermal skin test. However, the patch test at the site of a previous lesion shows a positive response in up to only 43% of cases2, and the positivity rate of patch test results using drugs other than nonsteroidal anti-inflammatory drug is very low3. Prick and intradermal skin test results are positive 24% and 67%, respectively. An oral challenge test with the suspected drug may be the best method, but it cannot often be performed because of its high risk. In the present case, the patient's voluntary provocation test aided the diagnosis of FDE. Only 5 cases of localized FDE due to cephalosporins including cefazolin, cephalexin, cefaclor, ceftazidime, and ceftriaxone have been reported. All cases were diagnosed by provocation tests and not by patch or intradermal test. To our knowledge, this is the first case report of cefaclor-induced generalized FDE. As cefaclor rarely causes FDE, patients as well as clinicians tend to ignore any skin lesions due to FDE. Furthermore, it is often difficult to identify the causative drug when patient is taking multiple medications. In summary, we report a case of cefaclor-induced generalized FDE proven by a self-rechallenge test.

 XML Download
XML Download