

 PDF
PDF Citation
Citation Print
Print



Dear Editor:
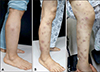
A 56-year-old female presented with erythematous nodules on arms and legs, which first appeared on legs two weeks prior (Fig. 1). The patient had not previously experienced similar symptoms. She had no specific medication, medical, or family history and showed no systemic symptoms. Routine blood examination showed no specific findings. Skin biopsy showed fibrous interlobular septum with widening and septal infiltrate by inflammatory cells, including histiocytes, lymphocytes, and eosinophils. Infiltrate extended to adjacent fat lobules near the septa. Von Kossa stain was negative (Fig. 2). Although the patient was administered pentoxyfylline, colchicine, zaltoprofen and prednisolone (10 mg/day), the number of lesions continued to increase (Fig. 1). Further investigations were conducted to identify the reason for treatment resistance. Laboratory tests showed an increase in lipase (14,139 U/L), α-fetoprotein (829.9 IU/ml), and carbohydrate antigen 19-9 (86.08 U/ml). Abdominal computed tomography showed malignant pancreatic cancer with metastasis to the liver and kidneys. The prednisolone dose was increased to 40 mg/day, but there was no improvement. She died of tumor lysis syndrome 5 days after diagnosis of malignancy.
Erythema nodosum (EN) can be idiopathic or secondary to infection, medication, inflammatory disease, or malignancy1. Although majority of cases associated with malignancy have been reported in relation to hematologic malignancies2, there are rare reports of EN secondary to solid tumors, such as lung cancer, colon cancer, and parathyroid cancer. Cases associated with pancreatic cancer are especially rare34. We were unable to find any reported cases of EN in pancreatic cancer patients in Korean literature. In the present case, the patient had no factors except pancreatic cancer that could have caused EN. Moreover, the patient developed EN at 56-year-old and showed no improvement in spite of over 2 months of appropriate treatment. There is no clear difference in clinicopathological features between idiopathic and paraneoplastic EN. It is difficult to distinguish between these two states by morphologic findings and distribution pattern. The most helpful clue is disease course and response to treatment. Paraneoplastic EN shows poor response to treatment and relapses more frequently than idiopathic EN. Chowaniec et al.1 reported that malignancy must be considered as a cause of EN in cases with clinical symptoms such as weight loss, age over 50 years and poor response to treatment. In pancreatic cancer patients with panniculitis, it is important to differentiate between EN and pancreatic panniculitis. It is clinically similar to EN, with erythematous nodules mostly appearing on the legs5. However, it can be differentiated from EN histologically due to the presence of a lobular panniculitis pattern with ghost cells, which occur when adipose cells lose their nuclei due to calcium deposits, leaving only an outline. Von Kossa stain can be used to identify calcium deposits, which was negative in the present case.
We experienced a rare case of EN in a patient with pancreatic cancer, and we believe this is the first report in Korea. This case shows the importance of considering possibility of malignancy, including pancreatic cancer, in cases of EN that do not show improvement following treatment.

 XML Download
XML Download