

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Palisaded neutrophilic granulomatous dermatitis (PNGD) is a rare pathohistologic diagnosis that has been associated with various autoimmune diseases1. However, to our knowledge, the occurrence of PNGD in patients with systemic sclerosis (SSc) /rheumatoid arthritis (RA) overlap syndrome has not been reported so far. There are many reports about skin manifestations of RA and SSc. However, reports about skin manifestations of their overlap syndrome are few. SSc-RA overlap syndrome is a rare autoimmune disease and has a distinct genetic, immunological, and clinical entity2. Herein, we report a case of PNGD in a patient with SSc-RA overlap syndrome.
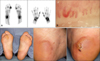
A 63-year-old woman presented with complaints of severe tenderness of both soles for 2 months. Symptoms developed after repeated heel walking as an exercise to improve muscle strength. About 6 years prior, she was diagnosed with interstitial lung disease. Approximately 1 year prior, she presented with hand and facial swelling and multiple joints pain. She complained of Raynaud's phenomenon and swollen hands. Sclerodactyly, telangiectases, and arthritis were also observed. The laboratory evaluation showed positive results for anti-Scl 70 antibody (Ab). The level of anti-cyclic citrullinated peptide Ab was 205.6 IU/ml and that of rheumatoid factor was 390.0 IU/ml. 99mTc bone scintigraphy showed abnormal increased joints uptake (Fig. 1A). Nailfold capillary microscopy showed a dilatated and tortuous capillary loops and giant capillary (Fig. 1B). The patient was diagnosed with SSc-RA overlap syndrome. When the patient was admitted with foot pain, 5-cm erythematous, annular tender edematous nodules were observed on both soles (Fig. 1C). The histopathologic findings revealed diffuse histiocytes infiltrations interstitially and palisading with neutrophils, nuclear dusts, and degenerated collagen bundles in the entire dermis (Fig. 2). Immunohistochemical staining for CD68 showed positive results for the infiltrated histiocytes. These findings were consistent with PNGD. We continued treatment for her underlying SSc-RA overlap syndrome, added dapsone 25 mg bid for PNGD. She was also advised to avoid weight-bearing activity and cold exposure. Soon after, the lesions seemed to have improved, but worsened 3 months later, prompting us to prescribe additional methylprednisolone and increase dosage of dapsone. About 5 months later, the lesions improved, but in the next 6 months she developed new lesions on both legs. A retrial of dapsone improved her skin within 2 weeks.
PNGD is a type of reactive granulomatous dermatitis associated with connective tissue diseases, lymphoproliferative diseases, and medications3. The lesion sometimes occurs after repeated trauma, and trauma may be involved in the deposition of immune complexes3. The differential diagnosis of PNGD includes small vessel vasculitis, neutrophilic dermatoses, granuloma annulare, and interstitial granulomatous dermatitis3,4. PNGD is known as a self-limiting benign disease, and management of the underlying disease is most important. Unlike other PNGD cases, this patient showed a waxing and waning clinical course. The reason for a different course may be that SSc-RA overlap syndrome has a greater disease burden than that in patients with limited SSc5. Although PNGD with SSc-RA overlap syndrome is very rare, clinical awareness of this combination would allow an early diagnostic and therapeutic approach.

 XML Download
XML Download