

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
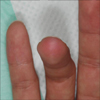
Hydrofluoric acid (HF) is one of the most corrosive acids and can produce progressive and serious tissue necrosis with severe pain1. Prompt first aid is mandatory to reduce damage after HF cutaneous exposure2. Herein we report a case of HF burn on a fingertip treated successfully with a single session of subcutaneous injection of small volume and low concentration of calcium gluconate. A 28-year-old man touched 50% HF last evening while he put experimental apparatuses in order in a laboratory. He washed his hands vigorously with soap and water, but the pain deteriorated as time went by. He visited our clinic about 15 hours after exposure of HF. Physical examination revealed a whitish vesicle with a diameter of 5 mm, which was surrounded by an erythematous flare on his right 4th fingertip (Fig. 1). He was given an injection of 6.7% calcium gluconate, 0.1 ml subcutaneously around the vesicle, which was made by diluting 10% calcium gluconate (2 g/2 ml Daihan Calcium Gluconate Injection®; Daihan Pharm Co. Ltd., Seoul, Korea) with saline in the ratio of 2:1. One day later, the severe pain subsided as well as the vesicle and edema improved moderately (Fig. 2). He did not experience any recurrence of pain and skin lesion over 40 days following-up. Unlike the damage caused by other acids that are rapidly neutralized, if untreated in HF burn, tissue destruction may continue for days, and result in permanent impairment3. The first and most critical treatment for an HF burn is immediate washing and cleansing of the affected area. The topical treatment is the second step, and it is much more effective if the application is started within 3 hours of the injury1. Subcutaneous injection of calcium agents partially overcomes the limitations of external application, especially the comparatively low skin penetrability2. However, the possible dangers of injecting of calcium gluconate solution into a small compartment such as finger may produce a sharp increase in tissue pressure, worsening of existing swelling and pain, impairing circulation and causing tissue necrosis3. Some researchers have suggested that subcutaneous injection should be reserved only for burns caused by HF acid of concentration above 20%, if there is a central grey wound with surrounding erythema, or in patients with severe throbbing pain4. In clinical practice, 10% calcium gluconate is recommended for used in topical injection treatment at 0.5 ml/cm2 and this quantity would neutralize 0.025 ml of 20%, 10 mol/L HF5. We injected calcium gluconate subcutaneously instead of external apply, because the patient contacted with high concentration of HF (50%), and had a whitish vesicle with erythematous flare with severe pain. We used 6.7% calcium gluconate which was lower than 10% (usual concentration in clinical practice) to minimize complication such as cellular damage or systemic electrolyte disturbances, and the outcome was favorable with no adverse effects. To date, there has been no widely accepted indication and protocol of subcutaneous calcium gluconate injection such as concentration, amount, and techniques in HF burn, and we think further studies are needed.

 XML Download
XML Download