

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Kaposi's varicelliform eruption (KVE) is a disseminated cutaneous infection caused by several viruses such as herpes simplex virus (HSV) type 1 and 2, and coxsackievirus A16 in patients with an underlying dermatosis. The term "eczema herpeticum" is used when the pathogenic virus is HSV1 or HSV2. KVE may rarely occur in patients with psoriasis; "psoriasis herpeticum" refers to the occurrence of KVE in psoriasis patients1,2. Here, we report the case of patient with erythrodermic psoriasis who developed KVE while receiving cyclosporine therapy.
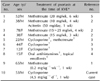
A 53-year-old male with a 30-year history of psoriasis vulgaris was admitted to our inpatient clinic with erythroderma starting 2 weeks earlier. Treatment with 4.5 mg·kg-1·day-1 cyclosporine A was initiated. On the 7th day of hospitalization, the patient developed vesicles and vesiculopustules all over the face, trunk, and extremities that progressed to papules with hemorrhagic crusts (Fig. 1, 2). A diagnosis of KVE was considered, and polymerase chain reaction (PCR) examination for HSV1 and HSV2 was performed; the result was positive for HSV1 infection. Bacterial culture from the lesions revealed no bacterial growth. Ocular investigation did not reveal a herpetic infection. Routine investigations including complete blood count, liver and renal function tests, and chest X-ray were normal. Therapy with intravenous acyclovir 10 mg/kg thrice daily was initiated and administered for 1 week. The lesions regressed completely within 10 days.
KVE is a potentially life-threatening viral infection that arises in pre-existing skin conditions3. Although majority of the cases occur in patients with atopic dermatitis, it has also been reported in other various diseases such as Darier's disease, Grover's disease, pemphigus foliaceus, and ichthyosis vulgaris1,2,3. However, KVE developing in a patient with psoriatic erythroderma is very rare1,2,3,4,5 (Table 1).
Although the exact pathogenesis of KVE is unclear, increased susceptibility to infections due to altered host defense and impaired skin barrier function are implicated1. Our patient had a compromised cutaneous barrier due to erythrodermic psoriasis. Furthermore, he was receiving systemic cyclosporine therapy, which might have predisposed him to the development of KVE owing to the drug's immunosuppressive effect.
Clinically, KVE presents as clusters of umbilicated vesicles that may transform into pustules or painful hemorrhagic crusted erosions on the skin affected by the pre-existing dermatosis2,3. This may be accompanied by fever, malaise, and lymphadenopathy2,4. Ocular involvement may be observed; and ophthalmology consultation should be performed immediately upon suspicion2.
The diagnosis of KVE is made clinically and can be confirmed by PCR for viral DNA or viral culture; electron microscopy and immunofluorescence testing can also be used1,2.
As systemic viremia with multiorgan involvement may cause morbidity and mortality in such patients, rapid diagnosis and antiviral therapy are important4. In summary, although rare, the diagnosis of psoriasis herpeticum should be kept in mind in psoriasis patients presenting with vesicular/vesiculopustular lesions.


 XML Download
XML Download