

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transplant pathology is an integral part of the comprehensive organ transplant programs. Experienced professionals with the expertise in pathology, immunology and molecular pathology take part in this core field. Transplant pathologists are now actively involved in many transplant related research projects as well as in pathologic diagnosis. The missions of transplant pathology are 1) to provide up-to-date and excellent laboratory diagnostic services for patient care, 2) to promote an academic activity devoted to education and training, and 3) to conduct basic and clinical research in transplant pathology.
In the renal transplantation, renal allograft biopsy is still a gold standard in the differential diagnosis of graft dysfunction. Today, it does not only mean to diagnose, but also to specifically grade and stage a disease entity and by this to provide prognostic information in order to guide a tailored treatment in the individual patient(1). The daily routine practice for renal transplant pathology is very important in terms of patient care, but how it is done in each hospital has not been thoroughly investigated in Korea. There are needs to establish informative and reproducible guidelines for standardization of graft diagnosis, and supporting systems for the improvement of diagnostic ability of the pathologists. As a first step to meet this needs, we surveyed current practices in handling renal graft biopsy and diagnosis to know whether any general guideline or supporting system could be established.
THE FIRST NATION-WIDE SURVEY FOR RENAL TRANSPLANT PATHOLOGY BY RENAL PATHOLOGY STUDY GROUP OF THE KOREAN SOCIETY OF PATHOLOGISTS IN 2016
To provide the continued excellence in the transplantation pathology laboratory, and to improve the diagnostic ability of pathologists for the best treatment of transplant patients, a nation-wide survey for renal transplant pathology was conducted by Renal Pathology Study Group of the Korean Society of Pathologists in 2016. This represents as a first investigation on the routine diagnostic practice of renal transplant pathology in Korea. There were only limited data documenting the current practice of transplant pathology across the domestic institutions.
A questionnaire was developed to understand the present status of transplant pathology practices in Korea. The first draft was sent to 10 pathologists of recognized experiences in renal transplant pathology to attain suggestions and criticisms that would contribute to constructing the final version. Through this work, a detailed questionnaire was finally made. This final questionnaire was sent to 46 renal pathologists, who were working in 46 different nationwide institutions. They were members of the Renal Pathology Study Group of Korean Society of Pathologists. This survey was e-mailed to the renal pathologists of each institution and all were preceded voluntarily.
We received replies from 33 out of 46 domestic institutions, corresponding to 71.7% response rate. A total of 32 questions were organized into three sections; 1) working conditions and status of institutions including the scale of pathology performance, the number and the competence of the working pathologists; 2) diagnostic criteria and reporting formats; 3) diagnostic difficulties and problems encountered by renal pathologists in daily routine practices. This study was approved by the Institutional Review Board (KC16QIMI0723) of Seoul St. Mary's Hospital, The Catholic University of Korea.
1. Institutional status of renal transplant pathology in Korea
The survey items about the institutional status including scale of pathology performance and competence of pathologists revealed a significant institutional variation in the scale, work load and experience of the pathologists.
A total of 33 institutions responded, 30 responses were from university hospitals (91%) and 3 (9%) were from general hospitals. Therefore, the survey was more a reflection of practices in university hospitals than other levels of hospitals.
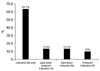
Renal transplant surgery and renal allograft biopsy were performed in 30 out of 33 institutions (91%). We asked the number of renal transplant surgery performed for a year before beginning the survey to estimate the scale of the transplant practices. The average number of renal transplant surgery was 49 cases/year, ranged from 5 to 322 cases/year. The number of renal graft biopsy that each institution diagnosed ranged from 3 to 411 cases/year and the mean was 70 cases/year (Fig. 1A). The number of renal graft biopsy handled by each institution varied greatly, and less than 25 cases/year were handled in more than half (53.6%) of the institutions in Korea. In only 7 institutions, the number of graft biopsy handled for a year exceeded 100 cases (Fig. 1B).
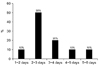
The number of the practicing pathologists for renal transplant diagnosis was not so different. In majority of the institutions (24/30, 80%), single pathologist was responsible for the diagnosis of renal graft biopsy. In remained other institutions (6/30, 20%), two pathologists were involved in the diagnosis. Largest portions of the pathologists (39%) were in the position of professor with a mean 23.5 years of experience on renal transplant pathology (Fig. 2A). The average years of experience of the responsible pathologists on the renal transplant diagnosis was 9.4 years. Most common experience of renal pathologists were less than 5 years (16/36, 44%), second were 5 to 10 years (11/36, 30.6%), and third were more than 10 years (9/36, 25%) (Fig. 2B).
Resident training system of renal transplant pathology in each institution was variable. The residents were working in 70% (21/30) institutions, but only 57.1% (12/21) institutions were able to provide education and training program for their residents. Though mean duration of renal transplant pathology training was 5.6 months (range 1.5 to 33 months), the residents in 75% (9/12) of the institutions which provide resident program were received less than 3 moths training in this field.
Communications between clinicians and pathologists, and timely diagnosis are important in the practice of transplant pathology. Many institutions (18/30, 60%) hold regular multidisciplinary conferences to discuss about the patients performed transplant biopsy. The average number of the conference was 29 times/year (range 2 to 250 times/year). Furthermore, clinicians themselves were actively participating in the diagnosis or review of renal graft biopsy by looking into slides through microscope directly.
Performance and timing of graft biopsy practice were varied among institutions. The following three types of biopsies were applied variously in each institution; 1) Protocol biopsy, taken at a certain time of stable graft function, 2) Indication biopsy, taken when signs of rejection happened, 3) Zero time biopsy, taken during the surgery. Only indication biopsy was performed in most institutions (63%, 19/30), but different mixture of biopsies (e.g. zero time+protocol+indication, zero time+indication, protocol+indication biopsy) were done in the rest of institutions (Fig. 3). The zero time biopsy was practiced in 8 (26.7%) institutions, and the protocol biopsy in 7 (25%) institutions. Protocol biopsy was taken in most of the large institutions that handle more than 100 biopsies/year (71.4%), and it's number varied from 1 to 3 times. The timing of the protocol biopsy was scheduled at different time points (2 weeks, 3 weeks, 6 months and/or 1 year after renal transplantation) in each institution.
Pre-diagnostic procedure (e.g. specimen fixation and staining) was relatively uniform among the institutions. Though 10% buffered formalin were used for fixation in most institutions (22/30, 73%), Duboscq-Brasil fixative (6/30, 20%), Bouin's fixative (1/30, 3%), and 15% buffered formalin (1/30, 3%) were also used. Periodic acid Schiff and trichrome stain were performed in all 30 institutions, and methenamine silver stain in 28 institutions.
Turn-around-time (TAT), that is days passed from receipt to diagnosis of renal graft biopsy, the most popular TAT was between 2 to 3 days in 50% (15/30) of institutions (Fig. 4).
Five institutions (17%) were providing a transplant pathology referral service to other hospitals. They handled average of 84 cases of renal transplant biopsies in a year (range 3 to 209 cases/year).
2. Diagnostic criteria and reporting formats of renal transplant pathology in Korea
All the respondent institutions had easy access to clinical information and 73% (22/30) institutions were receiving faxed or formal paper of request for the biopsy diagnosis.
For the diagnostic criteria of reporting the renal transplant biopsies, most recently updated of version of The Banff 2013 classification were used in most institutions (21/30, 70%), and Banff 2007 classification was the second most commonly used version (20%) (Fig. 5). As for the scoring of histologic changes, almost all institutions (28/30, 93%) were reporting Banff scores by the Banff classification.
As the diagnostic criteria of antibody mediated rejection (ABMR) and ancillary tests for its diagnosis have particularly changed a lot compared to other categories of rejection, we asked what test was used for the diagnosis of ABMR. C4d stain was used in 16 institutions, C4d and donor specific antibody test was conjointly used in 14 institutions. For the diagnosis of ABMR, 18 (60%) institutions chose immunohistochemical (IHC) staining method to confirm the deposit of C4d in renal biopsy, 9 (30%) chose both IHC and immunofluorescent (IF) staining method and 3 (10%) were using IF staining method (Fig. 6). There is no institution using gene expression profiling for the diagnosis of ABMR, so we could know that gene expression profiling was not yet incorporated in the routine renal transplant diagnosis in Korea.
SV40TAg IHC staining was also widely used to diagnose polyomavirus nephropathy (PVN); 18 (60%) institutions routinely examined polyomavirus by IHC in all renal graft biopsies, 9 (30%) examined selectively when PVN was suspected in routine stains, and 3 (10%) used no SV40TAg IHC in the practice.
Other IHC stains used for the renal transplant diagnosis by the pathologists were as follows: CD3 (2 institutions), CD3&CD68 (2 institutions), anti-Adenovirus stain (1 institution) and CD61 (2 institutions). Electron microscopy (EM) examination was done routinely in almost all institutions (28/30, 93%), and the remaining 2 institutions done EM when needed. When we asked whether they report incidentally found accompanying renal lesions, all 30 institutions answered that they diagnose the accompanying renal lesions including glomerulonephritis as well as transplant lesion and routinely perform EM and IF for such purpose also.
3. Diagnostic difficulties and problems of renal transplant pathology in Korea
In daily practice of the kidney transplant diagnosis, some of the pathologists complained of excessive workload, and some others complained of difficulty for accumulating experience due to a limited number of renal graft biopsies they encounter. Inadequate specimen, insufficient clinical information and short turn-around-time were also the difficulties that respondent pathologists were facing (Fig. 7).
Compared to general pathology, majority of the respondents (83%) answered that renal transplant pathology requires higher level of expertise and gives more burden to the pathologists. The character of the Banff classification was pointed out as one of the cause of burden, because it is composed of many subdivided elements such as Banff scores that need keen observation of histologic changes. Inter-institutional and inter-observer variations in renal transplant diagnosis were also revealed as a problem and they could be caused especially by detailed Banff scoring.
The pathologists with heavy working load expressed difficulties in meeting the short TAT and for the stress caused by insufficient manpower. On the other hand, pathologists who received small number of graft biopsy pointed out the difficulty in strengthening the expertise in transplant pathology. Young pathologists expressed frustration with the short experience and TAT and limited opportunities to learn about kidney transplant pathology during their residency.
4. A suggestion for the improvement and standardization of diagnosis on renal transplant pathology
Most respondents agreed that there are needs for standardized diagnostic practice guidelines, regular education on kidney transplant pathology, and convenient ways of consultation are required.
Suggestions by the respondents to improve the diagnosis of renal transplant biopsy are as follows; 1) compensation of right cost for renal graft biopsy since it demands very short TAT and more labor to the pathologists, 2) systematic support from the academic society and government to cultivate experts in the field of transplant pathology, 3) more detailed discussion between pathologists, 4) support for education, training and research specialized in renal transplant pathology, and 5) setting of standardized pathology request form detailing clinical information for the diagnosis.
To solve the problems found, we have conducted regular meetings and symposia for the improvement and standardization of renal transplant diagnosis for the members of Renal Pathology Study Group of the Korean Society of Pathologists. We are currently working toward the enhancement of the expertise of renal pathologists and to increase inter-institutional and inter-observer reproducibility by 1) production of a set of virtual slides for standardization of transplant diagnosis, 2) education by training virtual slides, 3) validation and gathering expert's consensus on diagnosis through virtual slides examination, 4) measurement of diagnosis agreement rate after examination, and 5) analysis of inter-institutional and inter-observer reproducibility.
DISCUSSION
This result shows laboratory handling of renal graft biopsy is reasonably standardized in Korea, according to a practical guideline for the renal pathology describing how to sample, process and report(2). They are practicing quite uniform and quality procedure from basic specimen fixation to ancillary tests. They were providing comprehensive array of studies for the optimum evaluation of renal biopsy. Also, most were having good communication with the nephrologists caring for the patients.
The pathologic diagnosis of renal transplant rejection is based on the most accepted classification, the Banff classification(3). Although all institutions in Korea were using Banff classification, about 30% were using outdated versions of the Banff. This result shows that a caution must be exercised when comparing biopsy results between institutions. During recent 20 years, new classification schema is announced and new entities are identified every other year, therefore it is not easy for the pathologist to keep up to date in this rapidly evolving renal transplant pathology.
Against our expectation, many respondents stated their opinion on the need for an education or consultation tool to enhance the inter-institutional and inter-observer reproducibility and to provide quality diagnoses in this area. Since renal transplant pathology is a very specialized and professional field of pathology, chance to see the renal transplant pathology is limited during residency training and also in academic meetings.
Moreover, many renal pathologists have limited chance to exchange their opinions with others or get feedback on their diagnosis because they are working solo in their institutions. Significant extra effort, time and expense are demanded of those desiring to remain current in their knowledge of transplant pathology. Since enhancement of inter-institutional and inter-observer reproducibility is obviously required( 4), more efforts of the academic society should be made to keep pace with the latest knowledge and deliver to the members.
A co-ordinated training system for renal transplant pathology could be one solution. Slide circulation and feedback system like “Histopathology external quality assessment schemes” in the United Kingdom(5) could be another option. As a first start, we are planning to develop on-line resources to learn and train the renal transplant pathology in a form of “Virtual Slide Atlas” (Fig. 8). Representative slides of renal transplant biopsy with different rejection or disease entities will be offered after reaching final consensus diagnosis. In that way, interpretational variations on ambiguous definitions or histologic variables could be reduced and under-experienced pathologists or training residents can use this “Virtual Slide Atlas” as a diagnostic reference.
CONCLUSION
We have suggested the standardization methods through the comparison of diagnostic classification systems and of the diagnosis formats by each institution in Korea. This survey provides comprehensive information on the domestic institutions, renal pathologists and issues of transplant pathology in Korea, which can be further used for the diagnostic improvement and quality patient care. Based on the collected information, we could further evaluate the observer variations among experts in renal transplant pathology and develop consensus reference slides to standardize the diagnosis.
We are currently developing “An Atlas of Renal Transplant Pathology by Virtual Slide System” which is an on-line reference resource to learn and train the renal transplant pathology effectively. It will contribute to the standardization of the transplant diagnosis and offer continuing opportunity to enhance the expertise of pathologist in renal transplant pathology in Korea.






 XML Download
XML Download