

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bicuspid aortic valve (BAV) is one of the most common congenital heart diseases, with an estimated prevalence of 1-2% in the general population.1)2) The clinical spectrum of BAV is quite broad, and most previous studies have focused on clinical complications of BAV including aortic valve (AV) dysfunction and aortic aneurysm.3)4)5)6)7)8) As the clinical importance of genetic traits associated with BAV has recently been re-investigated,9) regional or population differences could be factors affecting clinical phenotypes. Nevertheless, the majority of clinical data regarding BAV are derived fromWestern population.6)7)8) In addition, although the majority of studies have been focused on full-blown BAV disease,10)11)12) there are growing numbers of ‘healthy BAV carriers’ who are incidentally diagnosed due to the recent increase in echocardiography as part of routine screening.
Recently, we described the clinical characteristics of Korean patients with BAV who underwent AV surgery.13) As that research included only patients with severe aortic valvular dysfunction, the full clinical spectrum of BAV could not be adequately addressed. Moreover, it was a cross-sectional study without longitudinal follow-up data. Therefore, we constructed a prospective cohort of asymptomatic Korean BAV patients in a tertiary referral hospital. In this report, we describe the clinical characteristics and classify the pathways of initial BAV diagnosis in the real world. We also describe the progression of AV dysfunction and clinical outcomes during mid-term clinical follow-up.
METHODS
Study outline
Recruitment of study patients began in July 2014 through a web-based platform. Patients with BAV aged over 19 years who underwent comprehensive echocardiography at our institution and agreed to participate the registry were prospectively enrolled. Patients who had history of open heart surgery (OHS) for BAV before enrollment were excluded. A total of 232 patients were recruited and gave written informed consent during the period from July 2014 to February 2017. According to our study purpose, we excluded patients for whom ‘initial surgery’ was chosen as a treatment strategy. Based on the current American College of Cardiology/American Heart Association (ACC/AHA) guidelines,14) which recommend an interval of 6-12 months for reevaluation in patients with severe AS/AR (stage C), we excluded 60 BAV patients who underwent OHS for AV or aortic aneurysm within 6 months after enrollment, and also excluded 2 patients who presented with overt symptoms (dyspnea of NYHA class 3 and 4) at initial enrollment. Finally, 170 patients were included in an interim analysis of the progression of AV dysfunction and surgical events over a period of about 4 years. Patient visit and echocardiographic follow-up scheduling was done at the discretion of the attending cardiologist. Based on to the current ACC/AHA guideline,14) routine follow-up echocardiography was performed at intervals of 6-12 months in patients with severe AS/AR, 1-2 years in those with moderate AS/AR, and 3-5 years in those with mild AS/AR. The present study conformed to the ethical guidelines of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of Asan Medical Center. In patients with multiple repeated echocardiographic examinations, the baseline date was defined by the first echocardiography in which BAV was detected.
Definitions of terminologies
We classified reasons for the initial diagnosis of BAV in all study patients. The major categories included presence of clinical symptoms or signs, focused screening due to family history of BAV or other congenital heart disease, and incidental detection on echocardiography. In particular, the incidental detection category included a variety of echocardiographic screening types, which we specified as coincidental findings during the diagnosis of other cardiovascular diseases (e.g., angina or arrhythmia), preparation of non-cardiac surgery, and purely incidental findings during general health examinations. History of hypertension was identified in those who repeatedly presented with blood pressure ≥ 140/90 mmHg or who were diagnosed with hypertension by a referring physician prior to study enrollment and were undergoing life-style modifications or use of anti-hypertensive medication. History of diabetes was identified in those who presented with fasting serum glucose ≥ 126 mg/dL or were being treated with oral hypoglycemic agents or insulin. Dyslipidemia was defined as total cholesterol of ≥ 200 mg/dL or use of lipid lowering agents. Chronic kidney disease was defined in patients with glomerular filtration rate < 60 mL/min/1.73 m2 for more than 3 months.15) Coronary disease was defined in patients with previous coronary angiography that showed significant stenosis or who had typical clinical symptoms and were being treated with anti-angina medications. The severity of AV dysfunction was graded as none (trivial), mild, moderate, or severe for each case of aortic stenosis (AS) and regurgitation (AR) according to American Society of Echocardiography recommendations.16)17) Aortic dilation was defined as aortic diameter over 40 mm at any level. The classification of BAV morphology was performed using transthoracic echocardiographic images and transesophageal echocardiographic images (n = 54, 32%). As described in our previous study,10) the conventional system classified BAV according to patterns of cusp fusion: type 1, fusion between right coronary cusp (RCC) and left coronary cusp (LCC); type 2, fusion between RCC and non-coronary cusp (NCC); type 3, fusion between LCC and NCC. Type 4 was indistinguishable from type 2 or 3, but type 1 was rejected due to the separation between RCC and LCC (Supplementary Figure 1). The resulting dichotomous system was a simplified classification according to the direction of the fused cusps: BAV-CCF (coronary cusp fusion) and BAV-MCF (mixed cusp fusion). The clinical outcome analyzed in this study was defined as total surgical events, which was the composite of isolated AV surgery, combined AV with aortic surgery and isolated aortic surgery. We classified the main causes of AV surgery to identify the dominant AV dysfunctions. Cases with equal grades of AS and AR were defined as AS dominant. However, for cases diagnosed with definite infective endocarditis, it was considered the dominant surgical indication. The main cause of surgery on the aorta was determined according to the findings of echocardiography, computed tomography, and the surgeon's surgical record.
Data analysis
We presented categorical variables as numbers with percentages and continuous variables as mean ± standard deviation. Comparisons between paired parameters were performed with the Wilcoxon test. Event rates during follow-up were estimated by the Kaplan-Meier method, and compared by the log-rank test or Breslow test, as appropriate. The Cox proportional hazards model was used to evaluate associations of patient characteristics with surgical events. All reported p-values were two-tailed and p-values < 0.05 were considered statistically significant. SPSS version 22 (IBM Corp, Armonk, NY, USA) was used for statistical analyses.
RESULTS
Baseline clinical characteristics
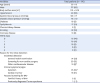
The mean age of the subjects was 50 ± 13 years and 117 patients (69%) were male (Table 1). The prevalence of hypertension, diabetes, and chronic kidney disease was 29%, 9%, and 1%, respectively. Thirteen patients (8%) had histories of coronary artery disease: among them, 6 had undergone percutaneous coronary intervention and 7 were receiving medical treatment only. Most (n = 154, 91%) had no or minimal dyspnea, and 16 patients (9%) had mild dyspnea of New York Heart Association (NYHA) functional class 2 at initial enrollment. Sixteen patients (9%) initially presented with NYHA class 2 but the attending cardiologists did not consider their symptoms to represent overt valve-related symptoms, and the patients were therefore managed with watchful observation. Among the reasons for the initial diagnosis of BAV, incidental detection was the most frequent (124 patients, 73%). Most cases were diagnosed during general health examinations (n = 91, 53%) or screening before non-cardiac surgery (n = 20, 12%), and incidental diagnoses occurred during evaluation for other cardiovascular diseases in 13 patients (8%). Twenty-five patients (15%) underwent cardiac evaluations due to subjective symptoms, and cardiac murmur was the reason for echocardiography in 18 patients (11%). Another minor reason for focused screening was family history (n = 3).
Table 1
Baseline clinical characteristics
Echocardiographic characteristics
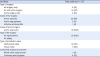
Regarding BAV morphologies, type 1 as defined by the conventional classification was the most common (n = 91, 54%) followed by type 4 (n = 37, 21%), type 2 (n = 34, 20%), and type 3 (n = 8, 5%) (Table 2). Meanwhile, using the dichotomous classification, we confirmed BAV-CCF in 91 patients (54%) and BAV-MCF in 79 patients (46%). Significant (moderate to severe) AS or AR was present in 77 patients (45%), whereas the remaining 93 showed no valvular dysfunction or mild AS or AR. Aortic dilation was present in 98 patients (58%). Two patients presented with combined congenital cardiac anomalies (atrial septal defect [n = 1] and patent ductus arteriosus [n = 1]).
Table 2
Echocardiographic characteristics

BAV: bicuspid aortic valve, CCF: coronary cusp fusion, LCC: left coronary cusp, LV, left ventricle, MCF: mixed cusp fusion, NCC: non-coronary cusp, RCC: right coronary cusp.
*Type 1, fusion between RCC and LCC; type 2, fusion between RCC and NCC; type 3, fusion between LCC and NCC; type 4, difficult to discriminate between type 2 or 3, while type 1 was clearly rejected due to the separation between RCC and LCC.
†BAV-CCF: coronary cusp fusion, BAV-MCF: mixed cusp fusion.
‡Moderate mitral regurgitation in one patient.
§Atrial septal defect (n = 1) and patent ductus arteriosus (n = 1).
Data shown are number (%) unless otherwise specified.
Surgical events during follow-up
During clinical follow-up of a median 4.0 years (interquartile range, 2.7 – 7.5), there were 2 deaths (pancreatic cancer in one patient with mild AS and subarachnoidal hemorrhage in the other with severe AS). A total of 27 patients (16%) underwent surgery for aggravated AV or aortic pathology: combined AV with aortic surgery in 12 patients (44%), isolated AV surgery in 11 patients (41%), and isolated aortic surgery in 4 (15%). Regarding the causes requiring AV surgery, AS was the most common underlying valvular dysfunction (n = 20, 87%) while the others included AR (n = 2, 9%) and infective endocarditis (n = 1, 4%). Aortic aneurysm was the cause of aortic surgery in all cases (n = 16, 100%) without aortic dissection or coarctation (Table 3).
Table 3
Summary of surgical procedures
The composite surgical event-free rate at 5 years was 89% ± 3%, and the individual 5-year event-free rate for isolated AV surgery, AV with aorta surgery, and isolated aorta surgery were 95% ± 2%, 96% ± 2%, and 98% ± 1%, respectively (Figure 1). Comparison of patient groups according to surgical events showed the surgery group (n = 27) was characterized by higher prevalence of dyspnea NYHA class ≥ 2, moderate or greater AS, and larger aortic root diameter at the tubular portion compared to the non-surgery group (Table 4). Regarding BAV morphology, the surgery group tended to present more frequently with BAV-MCF according to the dichotomous classification, compared to the non-surgery group (63% vs. 43%, p = 0.091) although the difference was not statistically significant. Regarding the impact of BAV morphology, the conventional classification did not clearly discriminate event rates between types (Figure 2A). However, using the dichotomous classification, patients with BAV-MCF tended to have a higher 5-year surgical event rate compared to those with BAV-CCF (18 ± 5% vs. 5 ± 3%, p = 0.036, Figure 2B). In univariate analysis, NYHA class ≥ 2, moderate to severe AS, BAV-MCF, and aortic root dilation were associated with surgical events (Supplementary Table 1). In multivariate analysis, moderate to severe AS (hazard ratio [HR] 4.61; 95% confidence interval [CI] 1.83-11.62; p = 0.001) and NYHA class ≥ 2 (HR 2.53; 95% CI 1.01-6.35; p = 0.048) were associated with the development of surgical events, whereas BAV-MCF (HR 1.75, 95% CI 0.77-3.96; p = 0.183) and aortic dilation did not remain significant (HR 2.13; 95% CI 0.87-5.21; p = 0.099).
Figure 1
Surgical event-free survival rates (A) and impact of severity of valvular dysfunction or aortic dilation at the time of the initial diagnosis (B-D). Ao: aortic, AR: aortic regurgitation, AS: aortic stenosis, AV: aortic valve.
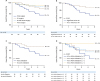
Table 4
Comparison of groups according to surgical events
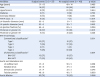
AR: aortic regurgitation, AS: aortic stenosis, BAV, bicuspid aortic valve, CCF: coronary cusp fusion, LCC: left coronary cusp, LV, left ventricle, MCF: mixed cusp fusion, NCC: non-coronary cusp, RCC: right coronary cusp.
*Type 1, fusion between RCC and LCC; type 2, fusion between RCC and NCC; type 3, fusion between LCC and NCC; type 4, difficult to discriminate between type 2 or 3, while type 1 was clearly rejected due to the separation between RCC and LCC.
†BAV-CCF: coronary cusp fusion, BAV-MCF: mixed cusp fusion.
Data shown are number (%) unless otherwise specified.

Progression of AV dysfunction
Follow-up echocardiography was available for 129 patients (76%) with a median interval of 3.9 years (interquartile range, 2.7 – 7.6 years). Overall, the severity of AS significantly increased during that period (p < 0.001, Figure 3A). Of 19 patients with moderate AS at baseline, 14 patients (74%) progressed to severe AS at follow-up echocardiography. Of the 61 patients initially diagnosed with mild AS, 6 patients (10%) progressed to severe AS and 15 patients (25%) to moderate AS. On the other hand, there was no significant change in the severity of AR during the same period (p = 0.361, Figure 3B). Among 19 patients with moderate AR at baseline, 7 patients (37%) had progressed to severe AR at the end of the study. Of the 16 patients initially diagnosed with mild AR, 3 patients (18%) progressed to moderate AR. However, there was no shift from mild AR to severe AR during an interval of about 4 years.

DISCUSSION
Ever since a one research group highlighted the large knowledge gaps regarding BAV,5) studies of BAV have proliferated during recent years. The American Association for Thoracic Surgery recently published a guideline for BAV aortopathy, which integrated studies about imaging, hemodynamics, and surgical treatment strategy.18) The BAV consortium recently published a genetic study,19) and some transcatheter AV replacement (TAVR) groups are now focused on BAV.11) However, natural history data based on long-term clinical observations are still lacking.
Two landmark studies met such requirements, the Toronto study7) and the Olmsted county study8) by the Mayo group. In particular, the Olmsted county study is an ideal community-based study, whereas our Korean BAV registry is affected by several source of bias because we included a referral cohort. Table 5 summarizes the differences between our cohort and the Olmsted county cohort. We believe that our study represents real world patients like those that clinicians in tertiary referral hospitals encounter during routine practice. For example, in contrast to the Olmsted county study, in which abnormal auscultation was the most common clinical condition (71%) associated with the first clue of initial diagnosis,20) the wide clinical application and availability of routine echocardiography in Korea can reveal different clinical situations associated with the first diagnosis of BAV. On the other hand, focused screening due to family history of BAV or congenital heart disease was conducted only in 3 patients in our cohort, while previous Western studies reported that familial clustering was involved in 20%-30% of isolated BAV cases21) and that the concordance among first-degree relatives of BAV patients was 6.4%.22) Therefore, our results raised the question of whether we provide appropriate patient education for screening of BAV during routine practice at our institution.
Table 5
Characteristics of the present study and the Olmsted County study

| Present study | Olmsted County study8) | |
|---|---|---|
| Nation / Ethnicity | South Korea / Asian | U.S. / Not specified |
| Study outline | Referral cohort of single center, prospective observational study | Community-based cohort, prospective observational study |
| Enrollment criteria | Exclusion of whom with previous AV surgery or AV surgery within 6 months after referral | No or at most mild AS or AR |
| LVEF ≥ 50% | ||
| No severe comorbidity | ||
| No complex congenital heart disease | ||
| Number of patients | 170 | 212 |
| Age (years) | 50 ± 13 | 32 ± 20 |
| Male | 69% | 65% |
| Most common reason for the initial detection of BAV | Incidental detection on echocardiographic screening (73%) | Cardiac murmur (71%) |
| AV function | No or mild AS or AR (55%) | No or at most mild AS or AR (100%) |
| Moderate or severe AS (22%) | ||
| Moderate or severe AR (19%) | ||
| Moderate or severe ASR (4%) | ||
| BAV morphology | RCC-LCC fusion in 54% | RCC-LCC fusion in 86% |
| Follow-up duration | Median 4.0 years (interquartile range, 2.7–7.5) | Mean 15 ± 6 years |
| Clinical outcome | 5-year surgical event rate, 11% + 3% | 20-year survival rate, 90% ± 3% |
| 20-year heart failure rate, 7% ± 2% | ||
| 20-year surgical event rate, 27% ± 4% | ||
| Changes in AV function | Significant aggravation of AS, but no difference in AR | Not described |
BAV is classified as an ‘at-risk’ stage according to the current ACC/AHA guidelines,14) but frequently persists as minimal to mild valve disease for a long time before clinical manifestations become apparent. Moreover, with the recent wide application of echocardiography in routine screening, growing numbers of ‘healthy BAV carriers’ are being detected in the patient population. Therefore, information about the natural history of BAV in patients with minimal or mild disease would be extremely valuable data for clinicians. The Olmsted county study included patients with minimal to mild BAV disease and obtained natural history data showing that 32% of patients underwent AV replacement and 13% developed new aortic aneurysms during a follow-up period of 16 years.20) Unfortunately, most studies conducted at research institutes suffer from inevitable selection bias because substantial numbers of patients already have moderate or greater BAV disease at the initial visit. As an alternative, data from the Mayo Clinic referral cohort seem more realistic.20) These data reflect patients referred to the Mayo Clinic outside Olmsted (n = 2824), including those with severe AS (12%), severe AR (8%), and aortic aneurysm (27%) at baseline.20) The Mayo Clinic referral cohort study revealed that 20-year overall survival in this group was significantly lower than that of the age/sex-matched general population (64% vs. 72%, p < 0.0001).20) We observed severe AS and severe AR at baseline in 12% and 9% of our cohort, respectively, percentages that were similar to the Mayo Clinic referral cohort. Although the Mayo Clinic data did not include event rates for anything other than survival, our data included a 5-year surgery rate of 12% ± 3% during follow-up.
One unique feature of our study was that it provides follow-up echocardiographic data for the patients in our cohort. The progression of AV dysfunction between baseline and follow-up echocardiography in our cohort was remarkable. The frequency of patients with moderate or greater AS significantly increased, from 26% to 43%. Among 96 patients with minimal to mild AS, 23 (24%) showed progression to moderate or greater AS. However, the frequency of moderate or greater AR did not significantly increase (from 26% to 29%) during the same follow-up period. Among 96 patients with minimal to mild AR, only 5 patients (5%) showed progression to moderate AR. Therefore, we observed a significant difference in progression rate between AS and AR. In the previous Toronto study, follow-up echocardiography (n = 619, interval of 7 ± 4 years) revealed no changes in AV velocity (2.3 ± 0.8 m/s to 2.6 ± 1.0 m/s).7) We hypothesize that the significant AS progression observed in our data was probably due to the higher mean age of the patients in our cohort (50 ± 13 years vs. 35 ± 16 years of Toronto study), and therefore calcific degeneration would be more likely to play an important role in the progression of AS. On the other hand, data regarding the progression of BAV-related AR are scarce. An analysis of one pediatric database indicates that AR grade tends to increase as subjects approach the age of 20 years.23) Therefore, we hypothesize that a mechanism other than calcific degeneration plays an important role in the progression of BAV-related AR. This interim result should be verified in a future study with longer follow-up duration.
The potential for population or geographic differences in BAV phenotypes is another interesting topic.24)-26) In previous Western studies, the frequency of BAV-CCF (or type 1 with RCC-LCC fusion) was the dominant phenotype with frequencies of 70 to 86%,7)8)12)27)28). Meanwhile, in Korea and Japan, the frequency of BAV-CCF is about 50%13)29). In this study, the frequency of BAV-CCF was 54%, which was quite similar to previously reported frequencies despite differences in enrollment criteria for BAV patients. Based on these results, we hypothesize that the distribution of BAV morphologies differs between Koreans and Western population. A more important issue is whether different BAV phenotypes affect clinical outcomes, which was previously suggested by the results of an embryological study.30) In the current study, with limited follow-up duration, patients with BAV-MCF tended to have more surgical events during follow-up than those with other BAV morphologies. Further investigations with longer follow-up duration are absolutely necessary to evaluate global patterns and clinical impact of BAV morphology.
Limitations
As this cohort was recruited in a tertiary referral hospital, the potential referral bias should be considered during interpretation of our data. Follow-up echocardiographic studies were performed in 76% of our cohort (129/170) and not in all patients, and the follow-up duration varied, resulting in a failure to perform quantitative assessments of progression of valvular dysfunction. The variability in follow-up duration parameters of valve dysfunction reflect patient evaluations based on the standards of routine clinical practice. Thus our data have limitations for use in quantitative assessments of the progression of valve dysfunction. Additionally, the median follow-up duration was only 4 years, which is not sufficient to represent the long-term natural history of early BAV disease.
Conclusion
In this initial prospective cohort study of BAV patients in Korea, we found that most patients (> 70%) were incidentally diagnosed with BAV, which reflects the wide availability of echocardiography in our medical environment. Although the patterns of BAV phenotype that we observed were different from those reported in Western countries, the clinical outcomes we observed were similar to those reported from a community-acquired cohort in the U.S. The potential impact of BAV phenotype on outcomes and patterns of progression of aortic valvular dysfunction (AS vs. AR) should be evaluated in further studies with longer follow-up durations.
 XML Download
XML Download