

 ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A parastomal hernia is a common complication in patients with stoma formation [1]. Many surgical approaches for repair of parastomal hernias have been described. But, the results have often been disappointing.
Recently, with further advancements in laparoscopic surgery, laparoscopic repair of parastomal hernias have been described with good results. Many investigations have been reported that laparoscopic repair of parastomal hernias with the proper technique can be safe, feasible and reliable. Furthermore, these kinds of repairs offer all of the well-known advantages of minimally invasive surgery [2,3].
However, despite many advances in laparoscopic surgery in Korea, there does not yet seem to have much experience in the treatment of laparoscopic parastomal hernia. In Korea, as far as we know, laparoscopic repair of a parastomal hernia with a modified Sugarbaker technique has not yet been performed. Herein, we present a case report of a patient suffering from a large parastomal and incisional hernias who underwent laparoscopic parastomal hernia repair with a modified Sugarbaker technique.
CASE REPORT
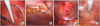
A 79-year-old woman, who had undergone an abdominoperineal resection for an adenocarcinoma (pT3N0M0, stage II) of the rectum 9 years ago, visited the emergency room with severe abdominal pain and vomiting. She was later diagnosed with a large parastomal and incisional hernias (Fig. 1). She first noticed the parastomal hernia seven years ago. In the past, she sometimes had difficulty with fitting stoma appliances and complained of discomfort due to the severe parastomal hernia. But, she was treated conservatively.
On preoperative abdominopelvic computed tomography (CT), a large parastomal hernia with concomitant incisional hernia was observed with a loss of fascia around her ostomy. Herniation of small bowel and greater omentum was observed (Fig. 2).
Although the patient experienced some improvement of symptoms with conservative management early in her hospital stay, the authors determined that a laparoscopic surgery for correction of the parastomal hernia would be necessary for long-term management.
Intravenous prophylactic antibiotics were given during induction of anesthesia, and the patient was operated under general anesthesia with endotracheal intubation. The patient was positioned supine with both arms alongside her body. The stoma was covered with a gauze and the stoma site was covered with a clean Ioban drape (3M, St. Paul, MN, USA).
Positioning of the surgeons, trocars and video equipment is shown is given in Fig. 3. Both surgeon and assistant stood on the side of the patient opposite to the stoma site. The first 12 mm balloon trocar intended for the camera was created with an open Hasson technique at the side opposite to the stoma, and a pneumoperitoneum was created with 12 mmHg of intraoperative abdominal pressure. Afterwards, a 30° angled, 10 mm scope was introduced. Next, a second 5 mm trocar was inserted subcostally. Finally, a third 12 mm trocar was placed just above the superior iliac crest (Fig. 3).
After complete lysis of adhesion with sharp dissection of the anterior abdominal wall, we measured the hernia defect and inspected concomitant incisional hernia (Fig. 4A). The parastomal hernia sac size was measured to be 7 cm × 5 cm and the concomitant incisional hernia sac size was 6 cm × 5 cm. The extent of the parastomal and incisional hernia defect were marked on the abdomen. A size of mesh was fit according to these marking such that it would be large enough to cover all hernia defects by at least 5 cm in all directions.
Before mesh application, the midline incisional hernia was closed with 1-0 Vicryl sutures using the Endo close Trocar Site Closure Device (Covidien, Mansfield, MA, USA) through separate small skin incisions (Fig. 4B). We used a 25 cm × 20 cm sized PARIETENE Composite mesh (Covidien) which was used as the original without cutting.
Orientation marks were made on the mesh and on the abdominal wall to allow for proper intraperitoneal orientation of the mesh. The first sutures were placed at the orientation marks before the mesh was inserted into the abdomen. The mesh was subsequently oriented using the orientation marks and the sutures were extracted through separate small skin incisions at the orientation marks with an Endo close Trocar Site Closure Device. The sutures were tied down to the anterior abdominal fascia, thus creating transabdominal fixation sutures.
We placed a transfascial fixation suture laterally in the mesh just above and just underneath the lateralized bowel (Fig. 4C) and more sutures were placed all around the mesh at its margins. Further fixation was performed with a mechanical fixation device-Autosuture endoscopic tacker (Endo Universal 65° devices, 4.8 mm stapler)-at the margin of the mesh with an interval of about 1 to 2 cm (Fig. 4D).
Total operating time was 340 minutes and there were no complications during the procedure (Fig. 5). At postoperative day (POD) #1, the patient started tolerating sips of water, and at POD #3, a soft diet was started. Following a brief ileus, the patient was discharged one week after surgery with no other complications. Now, 6 months after surgery, the patient has shown no evidence of recurrence (Fig. 6).
DISCUSSION
Parastomal hernias continue to be a common complication after stomal surgery [1]. Their rate of incidence varies between 4% and 48%. Although most asymptomatic hernias are well tolerated and can be managed conservatively, approximately 30% of hernias require surgical intervention for symptoms that include bowel strangulation, obstruction, bleeding, parastomal pain, poorly fitting appliances, and leakage [1].
Many different surgical approaches for repair of parastomal hernias have been described. The three most common surgical approaches are primary fascial repair, stoma relocation, and repair with mesh. Direct primary fascia repair at hernia site had reported recurrence rates of 38% to 100% [4], Additionally, stoma relocation does not remove the risk of parastomal hernia developing at the new stoma site and incisional hernia can still develop at the previous stoma closure site. A repair with mesh has shown improved results over stoma relocation and primary fascial repair [4].
Recently, with increasing research and advancement in laparoscopic surgery, a laparoscopic method for repair of parastomal hernias with mesh was described, with good results on short-term follow-up [2,3,5,6]. Laparoscopic parastomal hernia repair can be divided into two main groups: Keyhole techniques and Sugarbaker techniques. Keyhole techniques have been described in several different ways [3,5]. But, they all have an intraperitoneal mesh with a central hole to allow the colon or ileum to pass through the mesh to go to the stoma site. Sugarbaker techniques have no hole in the mesh, but rather the bowel going to the stoma is lateralized and covered by the mesh [6-8].
In 1980, Sugarbaker [7] first described an open technique for repair of parastomal hernia using an intraperitoneally placed polypropylene mesh [7]. In 1998, it was reported the first case on laparoscopic parastomal hernia repair with a "Sugarbaker technique" and in 1999, it was reported a case of a laparoscopic repair of a parastomal hernia with "Keyhole techniques" by Bickel et al. [9].
Modified Sugarbaker technique was first described by Stelzner et al. [10] in 2004. By laparotomy, an intraperitoneal expanded polytetrafluoroethylene mesh was placed with overlap the edges of the fascia by of at least 5 cm in all directions. In 20 patients, with a mean follow up of 3.5 years, they saw three asymptomatic recurrences.
In 2007, Muysoms [8] reported a "Laparoscopic modified Sugarbaker technique for parastomal hernia" in five patients with good early results, no early recurrences and good functional outcome.
In many investigations, it has been reported that laparoscopic repair of parastomal hernia is a safe, feasible and reliable technique offering the well-known advantages of minimally invasive surgery. However, despite many advances in laparoscopic surgery in Korea, there does not yet seem to have much experience in the treatment of laparoscopic parastomal hernia. It was no until 2005 that Lee et al. [5] reported laparoscopic repair of parastomal hernia using Keyhole-technique for the first time in Korea.
However, some reports using keyhole techniques have shown disappointing results with many recurrences [2,8]. For example, Safadi [2] reported a recurrence rate of 56% (5/9 patients) within 6 months of the operation. Muysoms [8] also reported a disappointing experience and high recurrence rates with the "Keyhole technique".
Recently, reports have shown that the Sugarbaker technique has lower recurrence rates compared to the Keyhole technique [6,8]. Muysoms [8] reported that laparoscopic parastomal hernia repair with "Keyhole techniques" had an unacceptably high recurrence rate. therefore, he changed to a "laparoscopic Sugarbaker technique" with more promising early results. Asif et al. [6] reported that the modified Sugarbaker technique may offer patients a significant decrease in the risk of recurrence with no significant increase in postoperative complications compared to other parastomal hernia repair techniques.
For incisional hernia, already laparoscopic treatment with the mesh is considered gold standard of treatment. For parastomal hernias, it seems that the global trend is shifting towards using a Sugarbaker technique rather than Keyhole technique.
In conclusion, we found that laparoscopic repair of a parastomal hernia with a modified Sugarbaker technique can be a safe and technically feasible. It is a mechanically logical technique combining the advantages of minimally invasive surgery with a favorable intra-abdominal pressure gradient. The viability of this approach, however, depends on longer-term follow-up reports with greater statistical power, and standardization of technical details.





 XML Download
XML Download