

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Liver transplantation is an established treatment modality for end-stage liver disease and hepatocellular carcinoma (HCC). With improvement in outcome, need for liver transplantation is in increase and far exceeds donation. Organ shortage can result in deleterious outcomes for recipients on the waiting list. Living donor liver transplantation (LDLT) has become an accepted procedure to shorten the gap between increasing demand and limited organ availability. Moreover, LDLT not only offered a significant survival benefit, but also reduced waiting time for recipients requiring urgent liver transplantation [12].
LDLT should be planned with a great caution because it also involves hepatectomy on healthy donor, and intraoperative abortion may harm both donor and recipient. Therefore, preoperative evaluation in LDLT involves both donor and recipient. It proceeds in a stepwise fashion in order to reveal any unsuitable condition as early as possible.
During 20 years of experience, we have updated our protocol to minimize any harm and avoid intraoperative abortion of LDLT. However, even with the most extensive and careful evaluation, there are situations where intraoperative abortion is inevitable in LDLT. Intraoperative abortion of donor hepatectomy for LDLT was reported to be close to 5% [3]. However, there has been no report of intraoperative abortion of LDLT including both recipient- and donor-related causes. Despite lowered overall incidence with accumulated experience, efforts to minimize intraoperative abortion may still be valuable. We report and share 15 cases of aborted LDLT among 1,179 cases.
METHODS
Study population and data collection
The present study was a single-center study. The study population was derived from the liver transplantation database from our hospital. Since the very first case of liver transplantation in 1996, we have kept track of every completed liver transplantation, and they were given with case numbers in numerical orders starting from one. Detailed medical data of over 1,800 liver transplantations have been stored and updated by both departments of surgery and anesthesiology. By contrasting the list of completed liver transplantation to the list of liver transplantations that have ever been scheduled on electronic medical record of our hospital, we identified 15 aborted LDLT among 1,179 cases performed from 1997 to 2016. The same screening process was independently performed by 2 different departments (surgery and anesthesiology) in order to avoid incidentally missed case. Medical documents of aborted LDLT were closely investigated. The Institutional Review Board at Samsung Medical Center approved the study (approval number: 2017-02-136-001), and waived need for individual consent.
Surgical indications, preoperative evaluation, and donor suitability
Surgical indications include end-stage liver disease. Patients, with unresectable and untreatable HCC with or without end-stage liver disease, were also indicated for LDLT. All patients with HCC were examined for metastasis using abdominal CT with or without magnetic resonance (MR) imaging, chest CT, and a bone scan with or without PET/CT. Imaging study was repeated until 1 month before LDLT to evaluate the suitability for liver transplantation with respect to the extent of tumor and hepatic vasculature. Our initial surgical indication of HCC was within the Milan criteria on radiological evaluation. However, due to the nature of LDLT, we have gradually expanded indication and included nearly all HCC other than major portal vein tumor thrombosis and extrahepatic metastasis [4]. For patients beyond the Milan criteria, an informed consent on tumor recurrence was obtained.
Every organ donation was absolutely voluntary, and sought no compensation other than helping recipients. Multidisciplinary evaluation process included blood tests, electrocardiography, pulmonary function test, and imaging studies. Blood tests include liver and renal biochemistries, complete blood count, coagulation profile, and serologic assays for viruses. Routine imaging studies were chest radiography, ultrasonography to evaluate liver quality, abdominal CT to assess liver volume and vascular anatomy, and magnetic resonance cholangiopancreatography (MRCP) to verify biliary anatomy.
The donor selection criteria were an adult younger than 65 years old, a body mass index (BMI) lower than 35, biochemistries within normal range, and adequate size of graft and remnant liver. In Korea, age over 16 years old is legally allowed as a donor, and recently, donors under 18 years old are approved after an additional consultation from Korean network for organ sharing. Our institutional policy is to recommend age over 20 years old, but donors between 16 to 20 years old with strong will were also accepted. Estimated graft volume greater than 40% of the recipient's standard liver volume was considered acceptable at the beginning of LDLT program, and our criteria were expanded, and an estimated graft volume greater than 30% is now considered acceptable. Donor hepatectomy was limited to 70% extent of the whole liver volume. Absolute exclusion criteria for donation were any medical conditions posing an increased perioperative risk and inoperable hepatic vascular variation. After confirming eligibility, biliary anatomy was verified, and predonation liver biopsy was selectively performed according to sonographic result. Suitability for organ donation is evaluated 2 months before transplantation except in emergent cases.
Details of the donor evaluation process have been modified over 20 years along with updates of diagnostic modalities. Doppler sonography was initially used to evaluate steatosis and vascular anatomy simultaneously. In 2007, CT angiography was adopted to verify vascular anatomy, and gray scale sonography was adopted for steatosis evaluation. Diagnostic modality for steatosis evaluation was then upgraded to the controlled attenuation parameter (Fibroscan; Echosens, Paris, France) in 2012. MRCP was adapted in 2007, originally to replace intraoperative cholangiography to verify biliary anatomy. Due to a long study period, various MR scanners were used. The baseline MR imaging was the recent 3T MR system (Intera Achieva; Philips Healthcare, Best, The Netherlands). From February 2015, a dual-echo mDIXON fat-water separation sequence has been introduced into the rouinte MR protocol to evaluate hepatic steatosis by using fat quantification. The mDIXON technique combines a 2-point DIXON method with the implementation of flexible echo times with following parameters: 3D T1-FFE sequence, 2-echoes: TE1 = 1.15 msec, TE2 = 2.30 msec, TR = 3.46 msec, Flip angle = 10, SENSE parallel imaging with acceleration factor 2.0 in phase-encoding direction.
Operative procedure
Living donor hepatectomy was initiated with open or laparoscopic incision. The intraoperative biopsy was performed to determine the suitability of organs for transplantation. During liver mobilization, the pathologic result was reported. Use of the graft was initially decided by an attending surgeon in the consideration of the intraoperative findings and the pathologic report.
Recipient hepatectomy was initiated with a bilateral subcostal incision with cephalic extension. The abdominal cavity was explored to check unreported seeding nodule, and quantify ascites. Standardized anesthesia was performed according to institutional liver transplantation protocol.
The starting time point of recipient anesthesia may vary considering the conditions of recipient and donor. Experts from both departments of surgery and anesthesiology discussed to decide the time point of recipient anesthesia in order to minimize operative duration. In this regard, our policy was updated to preceding recipient hepatectomy over donor hepatectomy in cases with possibility of abortion due to recipient.
RESULTS
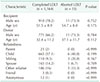
Demographic characteristics of completed and aborted LDLT are summarized in Table 1. Of 1179 LDLT, 15 cases (1.3%) were aborted. 5 cases were donor-related, and 10 cases were recipient-related. The incidences of every 5 years and the annual data for recent 5 years were provided in Fig. 1. Donor-related abortions were due to unexpected liver quality with steatosis in all 5 cases. Recipient-related abortions were related to unexpected disease progression in all cases, but they differ in details. As, we progress LDLT in a stepwise fashion, a final decision of aborting a case was made at a different stage of LDLT. All recipients of donor-related abortion were intubated, but further procedure was aborted before making a surgical incision, because living donor operation precedes recipient operation. However, in recipient-related abortion, donor operation was usually already progressed to some degree before abortion. Cholecystectomy was performed in 7 potential donors, and 3 cases were aborted after intubation, without making a surgical incision.
Unexpected liver quality
Characteristics of donors and potential recipients of these cases are summarized in Tables 2, 3. The first donor in this series had a mild elevation of liver enzyme (ALT: 76 U/L) and BMI slightly exceeding 25 kg/m2. A mild fatty liver was found on sonography, and preoperative liver biopsy was not performed. However, intraoperative frozen biopsy initially showed 70% microsteatsosis, and rebiopsy was done to show even higher degree of microsteatosis, which was over 90%. Including this case, preoperative liver biopsy was omitted in 3 donors with normal to mild fatty change on ultrasonography or MRCP. In these cases, results of intraoperative biopsy far exceeded our expectation based on preoperative evaluation. Preoperative liver biopsy was performed in 2 patients, and showed 7% and 30% macrosteatosis. In these cases with preoperative liver biopsy, results of intraoperative biopsy exceeded preoperative results, and rebiopsy were done in all cases to confirm the degree of steatosis. The intraoperative abortion was finally decided after discussing with liver pathologist and hepatologist, and during discussion, a surgical incision on the recipient was delayed. A donor, with high BMI, had one month of lifestyle intervention to lose weight before donation (27.7 → 27.4 kg/m2 in #1527). A liver-to spleen ratio was retrospectively calculated and showed inconsistent results.
Unexpected disease progression
Details of recipient-related abortions are summarized in Table 4. Among 10 cases of intraoperative abortion related to unexpected disease progression of potential recipients, five cases were related to extension of HCC. Three cases were found with multiple seeding nodules on peritoneal surface, rectal shelf and pelvic cavity. The remaining 2 cases were related to invasions to the distant organs, such as diaphragm, stomach and porta hepatis lymph nodes. An intraoperative photograph of distant metastasis on diaphragm is shown in Fig. 2. After confirming extensions of HCC by intraoperative frozen biopsy, intraoperative abortion was decided.
Results of preoperative evaluation in patients with HCC are summarized in Table 5. In all 5 cases, distant metastasis was not expected from preoperative evaluation. Tumor markers, such as α-FP, and CA 19-9 tests were routinely checked in every recipient. However, the degree of elevation was inconsistent in theses cases. Among 5 cases, 2 patients had a mild elevation of α-FP (59, 26.1 ng/mL), whereas 3 patients had extremely high levels (2,344, 45,367, 6,764 ng/mL). Three patients had residual lesions after transcatheter arterial chemoembolization. Remaining 2 patients had multiple lesions with variable sizes. PET/CT was used in all patients to evaluate distant metastasis. PET/CT showed no evidence of distant metastasis in 4 patients. In 1 patient, a metastasis in the left ilium could not be completely ruled out on PET/CT, and multiple seeding mass was found intraoperatively.
Unexpected disease progressions, other than HCC metastasis, were 2 cases with bowel inflammation with or without ischemia, 2 cases with severe adhesion, and 1 case of severe portopulmonary hypertension. A photograph of bowel inflammation with ischemia is shown in Fig. 3. Preoperative infection parameters, such as white blood cell count and C-reactive protein, in this patient were slightly raised (18.9 × 109/L, 6.73 mg/dL, respectively). In 1 case (#1303) with history of radiofreuency ablation, the patient showed a mild pulmonary hypertension (44/22, mean 28 mmHg) related to Budd-Chiari syndrome. The degree of pulmonary hypertension was acceptable for LDLT, but abortion was decided considering the risk of hemodynamic instability related to adhesion and pulmonary hypertension. A severe adhesion was expected in a patient (#1347) with a history of prior extended hemihepatectomy performed 10 years before LDLT. However, the degree of adhesion far exceeded our expectations and acted as a barrier in providing an adequate surgical field. Abortion was decided before massive bleeding considering difficulty in recognizing anatomy for inflow and outflow reconstruction. One case was related to severe portopulmonary hypertension. After anesthetic induction, high pulmonary artery pressure was noticed via pulmonary artery catheter (82/38, mean 58 mmHg). After discussion between the experienced attending surgeon and anesthesiologist, intraoperative abortion was decided, and delayed until mean pulmonary artery pressure is decreased under 35 mmHg. On preoperative echocardiography, minimal tricuspid regurgitation and pleural effusion made it difficult to accurately predict pulmonary hypertension.
Retrospective medical record review
Authors performed careful and detailed reviews of all 15 cases in this series, in order to identify any patterns to help predicting intraoperative abortion. We categorized intraoperative abortion according to reasons. However, there was no pattern observed. Despite updates of our routine practice, remaining limitations of radiologic and laboratory evaluations showed that unpredictability is always possible.
Postoperative course
All donors of intraoperative aobrtion had an uneventful postoperative course, and were discharged at an average of postoperative day 8. Long-term complication was not reported, regardless of surgical incision or cholecystectomy. Steatosis of liver was treated with lifestyle intervention, such as abstaining from alcohol and dietary restrictions.
Consequences of recipients were somewhat deleterious. Seven out of 10 recipients in recipient-related abortion, and 1 out of 5 recipients in donor-related abortion expired within 1-year follow-up. One recipient survived for 4 years, and became loss of follow-up. The shortest survival duration among expired recipients without further transplantation was 1 day, and 6 years was the longest survival duration. Retrials of transplantation were performed in 4 recipients, and they showed successful outcomes. For retrials, donations were from different donors in 3 cases related to steatosis, and the donation was from the same donor in 1 case initially aborted due to a severe portopulmonary hypertension.
DISCUSSION
In the present series, we exclusively reported intraoperative abortion of LDLT. The overall incidence was 1.3% (15 of 1,179) in 20 years. Among 15 cases, 5 cases were donor-related, and 10 cases were recipient-related. No donor from intraoperative abortion suffered from postoperative complication. Although LDLT is a widely performed procedure, limited data on the incidence and consequences of intraoperative abortion exist. Twenty years of experience and decision making of a large volume center are reflected in this study.
LDLT now plays a key role in the treatment of end-stage liver disease and HCC, especially in Asian countries where deceased donor is limited. However, as LDLT takes risk of general anesthesia and donor hepatectomy on healthy individuals, selection and safety of donor have been paramount concern. Despite large variations in donor selection criteria from center to center, one thing common is that donation must always be decided voluntarily without any coercion. Our center previously demonstrated the safety of donor hepatectomy, and identified risk factors associated with donor complication. In our previous analysis of 827 LDLT, 90% of donors experienced no complications, and among 10% of donors with some complication, progression to death or permanent illness was not reported [5].
Five cases of abortion were donor-related. A previous study has reported that the overall incidence of intraoperative abortion of living donor hepatectomy was 12 cases out of 257 cases (4.7%) [3]. In previous series, 7 cases were due to anatomical variations, and 3 cases, including 1 case of steatosis, were related to unexpected liver quality. The remaining 2 cases were related to intraoperative events. The overall result far exceeded our rate of donor-related abortion (12 of 257, 4.7% vs. 5 of 1,179, 0.42%). The difference is mainly driven by abortion due to anatomical variation (7 of 257, 2.7% vs. 0 of 1,179, 0%), because none of intraoperative abortion, in our report, was associated with biliary or vascular anatomical variation [3]. Anatomical variations of vascular and biliary structures are relatively common, and show ethnic difference [6]. It has also been reported that most of anatomical variations other than intraparenchymal origin of anterior portal vein can be safely managed with intraoperative assessment and technical modification [7]. In our center, preoperative MRCP has been adopted, and routinely used for donor evaluation since 2007 to replace intraoperative cholangiography. Despite advancements in MR imaging, the accuracy of preoperative MRCP is still insufficient compared to intraoperative cholangiography [89]. However, MRCP has advantage of visualizing biliary anatomy preoperatively. All of anatomical variations were preoperatively screended, and variations detected during and before donor hepatectomy seemed acceptable.
All 5 cases of donor-related abortion were due to steatosis. This result is consistent with the previous report, with 1 intraoperative abortion out of 257 (1 of 257, 0.39% vs. 5 of 1,179 0.42%) [3]. Although livers with more than 30 % of macrosteatosis has traditionally been excluded from donation, many centers have accepted 30% to 60% of macrosteatosis in deceased donor type to relieve organ shortage [10]. However, situations for LDLT are totally different, because steatosis is strongly associated with small-for-size syndrome [11]. As mentioned above in the method section, our institutional diagnostic modalities and guidelines for steatosis have continuously been upgraded. In the beginning, Doppler sonography was initially used, and mild to moderate steatosis was indicated for preoperative liver biopsy. In 2007, sonography was specified, and converted to gray scale liver, gall bladder and pancreas sonography, and since then, more than moderate steatosis was indication of liver biopsy. In patients with more than 30% macrosteatosis confirmed in biopsy, lifestyle intervention was applied for at least 30 days, and rebiopsy was done afterward. Fibroscan, a controlled attenuation parameter was adopted in 2012. It is ultrasound-based non-invasive tool to assess steatosis. It is validated in various liver diseases, such as viral hepatitis, biliary disease, and alcoholic and non-alcoholic disease [12]. Since 2015, MR images from MRCP have been used in steatosis evaluation under consultation of department of radiology. One case was aborted due to steatosis at the beginning of MRCP adoption, and intraoperative abortion related to steatosis has never been observed since then.
Distant metastasis of HCC were the most common cause of recipient-related abortion. Unlike strict Milan criteria for deceased donor liver transplantation, extended indication for LDLT is applied for patients with HCC. Survival benefit of liver transplantation in patients with HCC beyond the Milan criteria has been previously reported [1314]. Although contribution of tumor diameter, number of nodules and microscopic vascular invasion on recurrence rate is still on debate, LDLT may be virtually the only option for patients with HCC exceeding the Milan criteria. Especially in the era of MELD-Na (model for end-stage liver disease with sodium) score based allocation policy, number of dropout cases from the waiting list is in increase [15161718]. Moreover, despite advancement in diagnostic modality, some reports suggest that preoperative number of nodule are under or overestimated [1920], and tumor markers also showed inconsistent results. For patients with HCC, our center has adopted preoperative MR imaging, which has shown to be effective in stratifying the risk of tumor recurrence in patients either within or beyond the Milan criteria [21]. However, distant metastasis in this series was undetected during preoperative evaluation even with radiologic assessments within a month before LDLT in all cases.
A severe portopulmonary hypertension, defined as mean pulmonary artery pressure over 50 mmHg, carries a significant perioperative risk, and limits the quality of postoperative outcome [22]. Unfortunately in many patients, it is not diagnosed until pulmonary artery catheter is inserted during general anesthesia [23]. Although preoperative echocardiography has been evaluated in every recipient, it has clear limitations as follows; First, it is not easy to measure systolic pressure of right ventricle in patients with minimal tricuspid regurgitation Second, in patients with increased pulmonary pressure, it is not easy to differentiate pulmonary hypertension from hyperdynamic state accompanied by end-stage liver disease. In our case, the patient was successfully treated with 10–15 ppm of nitric oxide after intraoperative abortion, and liver transplantation was rescheduled after mean pulmonary artery pressure was decreased under 35 mmHg.
Preventability is the last, but not the least issue. Intraoperative abortion of LDLT should be minimized, considering the risk of healthy donors and deleterious outcome of the recipients. As mentioned above, our center has continuously adopted new modalities and upgraded evidence-based guidelines. These efforts were not only focused on improving clinical outcome, but also on minimizing intraoperative abortion. With clear limitations of the radiologic and biochemical assessments of donors and recipients, we have also modified our routine practice. In recipients highly suspicious of abortion, such as HCC extension or pulmonary hypertension on preoperative echocardiography, we start recipient operation before donor hepatectomy. As a result, some of latter recipient-related abortion avoided a surgical incision in donors. Despite these efforts, the rate of intraoperative abortion of LDLT did not decrease in our center, and it is clear that there still remain questions on a measure to minimize inevitable abortion. This may be related to the expansion of surgical indication of LDLT in patients with HCC, and the most of latter aborted cases were due to unexpected progression of HCC. Considering that LDLT is virtually the only option for these patients, complete prevention of intraoperative abortion may not be feasible in LDLT. However, with continued improvements in the preoperative evaluation technique, the incidence of aborted LDLT should and would decrease.
Limitation is that we categorized series of cases according to the reasons of abortion, but failed to present any pattern that would be helpful in predicting an abortion. It may be due to the small number of cases in each category, but it also clearly shows limitations of preoperative evaluation. Unlike strict nationwide surgical indications of deceased donor liver transplantation, indications and guidelines of LDLT might vary from case to case, and have been widened with strong will of donors. Sharing an experience of intraoperative abortion of LDLT in a large-volume center is valuable, even in the absence of preponderant pattern. In this regard, we report and share our experience of aborted LDLT in 20 years.
In conclusion, at our single, large-volume center study, the rate of aborted LDLT was 1.3%. Further efforts to decrease it with preoperative evaluation should be made.







 XML Download
XML Download