

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the prevalence of gastric cancer has recently decreased, it remains the third leading cause of cancer-related death [1]. This means that many patients still die due to incurable gastric cancer. In general, curability cannot be expected for metastatic gastric cancer [2].
However, some patients with metastatic disease show remarkably long survival [3456]. Although such outcomes might be caused by aggressive treatments [78], it is necessary to evaluate the other clinicopathologic factors that can affect the prognosis of such patients. With respect to this issue, it is remarkable that metastatic gastric cancer includes two heterogenous disease categories.
Based on whether curative resection was previously performed or not, metastatic gastric cancer can be classified into the 2 disease categories. One is initially metastatic disease with M1 factors, and the other is recurrent metastatic disease in which curative gastrectomy was previously performed. Each disease category is known to have a poor prognosis. In particular, initially metastatic disease is a representative feature of poor prognosis. According to data from the National Cancer Institute [9], the 5-year survival rate was 4.0% in patients with stage IV gastric cancer. Likewise, a good prognosis is also unlikely in patients with recurrent metastatic gastric cancer, despite the performance of previous curative surgery [101112]. Based on such previous reports, many physicians tend to regard both type of metastatatic disease as having similar prognosis. Therefore, they have been managed both disease categories with chemotherapy alone. However, there has been no evidence to support such a similar treatment for both disease categories.
Some investigators described that surgical resection might cause a favorable prognosis through reduction of tumor-burden [13141516]. Considering these reports, recurrent metastatic gastric cancer is expected to have a smaller disease-burden than initially metastatic disease, because curative gastrectomy was performed before. Although chemotherapy can also lessen the disease-burden of initially metastatic disease, gastric lesions do not always show a dramatic response to chemotherapy. Even when tumors respond to a specific regimen, most eventually encounter drug resistance. In addition, remaining gastric tumors often lead to some critical problems, which may play a definite role in heightened mortality [1718].
On the other hand, there are contradictory opinions regarding surgical treatment [192021]. Reports in which surgery was recommended for stage IV gastric cancer have been criticized, because the candidates for surgical resection might have a smaller disease-burden or better performance status than the other patients with metastatic diseases [22]. In addition, while surgical treatment could reduce the disease-burden of advanced gastric cancer, dispersion of cancer cells into the peritoneal cavity may result [23]. With regard to such findings, initially metastatic gastric cancer might be associated with a better prognosis than recurrent metastatic disease, in which an unfavorable condition can be induced by previous surgery.
Based on these previous opinions, we established a hypothesis concerning the treatment strategy for stage IV gastric cancer. Although the previous investigators did not reach a consensus on the prognostic effect of surgery, a distinct difference between initially and recurrent metastatic gastric cancer was whether gastrectomy was performed or not. Therefore, the behavioral difference between the 2 disease may correlate with the prognostic effect of gastrectomy in stage IV disease.
In this study, we compared the prognosis and cause of death between patients with initially and recurrent metastatic gastric cancer in order to understand how gastrectomy affects the prognosis of stage IV disease.
METHODS
Between January 2006 and September 2013, the patients who underwent chemotherapy alone for metastatic gastric cancer at Korea University Ansan Hospital, South Korea were enrolled in this study. Enrolled cases satisfied the following criteria: (1) pathologically proven gastric adenocarcinoma, (2) considered to be M1 stage at the initial diagnosis or underwent metastatic recurrence after curative gastrectomy, and (3) without other malignancy other than gastric cancer.
We collected records containing information regarding the clinicopathologic characteristics and treatment outcomes from those enrolled in the study. Patients were divided into 2 groups: Initially metastatic gastric cancer (IM) group and recurrent metastatic gastric cancer (RM) group. IM group included patients underwent chemotherapy for metastatic gastric cancer at the initiall diagnosis, and RM group included patients who underwent chemotherapy for metastatic recurrence after curative surgery (The patients with gastric stump recurrence were excluded from RM group). Clinicopathologic outcomes including age, sex, serum CEA level, serum CA 19-9 level, degree of differentiation (by World Health Organization classification), distant lymph node metastasis, bone metastasis, lung metastasis, liver metastasis, carcinomatous peritonei, frequency of transfusion, frequency of chemotherapy, and dose reduction of chemotherapeutic drugs were investigated in each group. Clinicopathologic characteristics and causes of death were compared between the 2 groups using the chi-square test and independent Student t-test. Additionally, overall survival was calculated and compared between the 2 groups by using Kaplan-Meyer method. Univariate and multivariate analyses were performed to investigate the significant prognostic factors using the Cox proportional hazard model.
IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA) and R software ver. 2.15.2 (The R Project for Statistical Computing; available at http://www.r-project.org/) were used for statistical analyses.
This study was approved for research on human subjects by the Institutional Review Board of Korea University Ansan Hospital (approval number: AS16144).
RESULTS
Patient demographics and clinicopathologic outcomes
A total of 170 patients were enrolled in this study. The mean follow-up time was 336.9 ± 303.4 days (range, 6–2,207 days). Of these patients, 104 were included in IM group and 66 in the RM group. The scheme of enrollment is showed in Fig. 1.
The clinicopathologic characteristics of 2 groups are compared in Table 1. The 2 groups showed statistically significant difference in several factors: serum CEA level, presence of distant lymph node metastasis, presence of liver metastasis, frequency of chemotherapy cycles, number of cases underwent dose reduction.
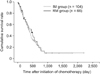
Comparison of overall survival between the IM and RM groups
Overall survival of the IM group did not differ from that of the RM group (P = 0.569) (Fig. 2).
Causes of death in the IM and RM groups
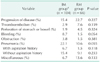
In the comparison of the causes of death, the IM group had a greater tendency to die of bleeding (P = 0.054) or pneumonia (P = 0.055) compared to the RM group did (Table 2).
As a supplement analysis, when pneumonia was further classified into ‘aspiration pneumonia’ and ‘nonaspiration pneumonia’, the IM group included 7 cases (6.7%) of aspiration pneumonia and RM group 1 case (1.5%). However, this difference was not statistically significant (P = 0.118) (Table 2).
Prognostic factors affecting overall survival in IM and RM groups
In multivariate analysis, bone metastasis (P < 0.001; HR = 2.847), carcinoma peritonei (P = 0.047; HR = 1.766), and the frequency of chemotherapy (P < 0.001; HR = 0.777) were significantly associated with overall survival of IM group (Table 3). In RM group, the serum CA 19-9 level (P = 0.012; HR = 1.000), the frequency of transfusion (P = 0.034; HR = 1.044) correlated with overall survival (Table 4)
DISCUSSION
In the current study, behavioral differences were compared between patients with initially and recurrent metastatic gastric cancer. As a result, survival did not differ between the 2 disease categories (Fig. 2); however, the 2 disease categories showed different tendencies regarding causes of death (Table 2). Although a P-value greater than 0.05 provided limited significance, the patients of IM group had greater tendency to die from bleeding or pneumonia than did RM group. We contemplated that this tendency might be caused by the remaining gastric lesions of IM group. In fact, as initially metastatic cases did not undergo gastrectomy before, they embed the potential to cause the following complications: First, the remaining gastric lesion of initially metastatic case is at a high risk of bleeding or perforation. Second, if the gastric lesion grows enough to cause obstruction or stasis, the patient is predisposed to aspiration pneumonia [24,25,26,27]. Our data also included more patients who died of aspiration pneumonia in IM group, even though comparative analysis did not reach a statistically significant difference (Table 2).
On the contrary, RM group was free from the gastric lesions, since we excluded the patients with gastric stump recurrence from this study (Fig. 1). Consequently, these patients might rarely encounter clinical crisis such as primary tumor bleeding, gastric outlet obstruction, and gastric perforation. In regard to these issue, we previously reported that ‘noncurative surgery’ delayed the time at which palliative procedures (e.g., endoscopic bleeding control or stent insertion) should be performed [28]. Therefore, when focusing on our results regarding causes of death, noncurative surgery can be a solution for stage IV gastric cancer [2829].
However, we failed to explain how surgery affects the prognosis of initially metastatic cases. Most of all, the previous history of gastrectomy did not cause any survival gain of recurrent metastatic cases, as we found no prognostic difference between IM and RM groups. In addition, when we investigated the clinical courses of stage IV patients who died of bleeding or pneumonia, these cases also embedded other mortality-related conditions regardless of gastric lesions (data not shown). Therefore, we should find the other factors that affected the prognosis in each group.
As shown in Tables 3 and 4, bone metastasis, carcinoma peritonei, and frequency of chemotherapy were revealed as significant prognostic factors in the IM group, while these factors had no significant prognostic effect in the RM group. Although both disease categories similarly showed incurable features, different prognostic factors affected each disease. In addition, even though the remaining gastric tumor increased some types of cancer-related death in the IM group (Table 2), the prognostic effect of such mortalities might be overwhelmed by the heavy “disease-burden” (e.g., bone metastasis or carcinoma peritonei). In other words, disease-burden may have a more significant effect on the prognosis of stage IV disease than noncurative gastrectomy.
Moreover, frequency of chemotherapy also attracted attention as a strong prognostic factor in the IM group (Table 3). In particular, it was inspirable that “dose reduction” or “number of chemotherapy lines” was not a significant prognostic factor. This result implied that the steady performance was the most important factor in chemotherapy for stage IV gastric cancer.
Considering all these results, we can contemplate a principle of planning treatment strategies for stage IV gastric cancer.
As indicated in the previous reports, some investigators assure as if palliative gastrectomy induces survival gain in initially metastatic gastric cancer [13141516]. However, as shown in our results, the benefit of noncurative surgery could not outweigh the prognostic effect of disease-burden. Although noncurative gastrectomy improved the general condition in some cases, an impellent surgery may cause a fatal mistake of delaying chemotherapy in patients with bone metastasis or peritoneal seeding. With regard to this issue, the recent results of a randomized controlled trial also showed that noncurative surgery can decrease chemotherapy compliance without any prognostic benefit [30]. Furthermore, according to our data, the type of noncurable factor was significantly correlated to the prognosis of stage IV disease. Therefore, disease-burden should be prioritized in planning treatment strategies for stage IV gastric cancer.




 XML Download
XML Download