

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
An isolated visceral artery dissection refers to the absence of an aortic dissection at initial presentation and the risk factors for an arterial dissection [12]. Single dissection of the visceral arteries are infrequent [34]. Multiple spontaneous isolated dissections of the visceral arteries are therefore considered extremely rare [256]. We report a case of multiple spontaneous dissections involving the superior mesenteric artery (SMA), the celiac artery (CA) and bilateral renal arteries (RA). The patient underwent endovascular intervention and conservative treatment and remains uneventfully until 84 months of follow-up.
CASE REPORT
Based on Inha University Hospital Institution's Policy, the Institutional Review Board is waived for case report. A 55-year-old man admitted to the Emergency Department due to a 7-day history of diffuse abdominal pain and nausea. Pain started after drinking alcohol, followed by vomiting, diarrhea, and bowel distension. On admission, he was generally weak, alert and hypertensive (160/80 mmHg). Other vital signs were within normal range. He was previously healthy and was not taking any medication. He denied past surgical history, allergies, smoking and previous hypertension but admitted frequent alcohol consumption for years. On physical examination, diffuse abdominal tenderness and hyperactive bowel sounds were noted. Blood analysis revealed a raised white blood cell count (15.35 × 109/L) with a predominant neutrophil level (83%). Laboratory tests noted to include elevated lactate dehydrogenase (LDH), D-dimer, C-reactive protein, serum creatinine, and aspartate aminotransferase. Pancreatic enzymes, rheumatoid factor, antinuclear antibody, antineutrophil cytoplasmic antibody and immunoglobulin levels were all within normal limits. A urinary analysis was negative.
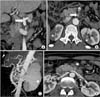
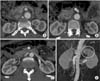
The computed tomography angiogram (CTA) demonstrated multiple spontaneous arterial dissections involving the proximal CA, SMA, and bilateral RA with subsequent focal renal infarctions (Fig. 1). The true lumen of the proximal SMA was markedly collapsed due to a large amount of thrombus formation in the false lumen (Fig. 1B). There was no sign of aortic aneurysm or atherosclerosis. The patient was admitted to the intensive care unit for close monitoring. Intravenous unfractionated heparin, beta-blocker and nonsteroidal anti-inflammatory drugs were administered. After a multidisciplinary discussion on day 3, endovascular intervention was indicated because the abdominal pain worsened. Multiple dissections were confirmed on angiograms (Fig. 2). A stiff guide wire was then introduced to the SMA, followed by the deployment of 2 balloon-expandable stents (Omnilink, Abbott Vascular, Santa Clara, CA, USA), 8 mm × 4 cm and 7 mm × 3 cm. The right renal infarction was considered for conservative treatment because the dissection was of segmental level (Fig. 2B). The left renal arteriogram demonstrated dissection and narrowing at the bifurcation level of the anterior division and the superior segmental artery included a corresponding perfusion defect at the upper pole (Fig. 2C). Stenting was promptly applied to improve renal perfusion and recovery as well as to prevent further renovascular hypertension. A 7-F sheath was exchanged to accommodate the guiding catheter, followed by the deployment of another balloon-expandable renal stent, 6 mm × 2 cm, at the level of a bifurcation to the anterior division. The pain significantly decreased the day after and the analgesia was eventually ceased. His blood pressure returned to a normal range and only oral antihypertension medication was prescribed. Laboratory tests were within normal ranges. CTA obtained at day 6 demonstrated good patency of the stents (not shown). Considering the severity of multiple arterial dissections, the patient was sent home on a regimen of Aspirin 100 mg/day and Warfarin 5 mg/day for 6 months, then replaced by a dual antiplatelet of Aspirin 100 mg/day and Plavix (Clopidogrel, Handok, Seoul, Korea) 75 mg/day during 4.5 years. Follow-up CTAs were obtained regularly. The latest CTA revealed good patency of the stents (Fig. 3), thus, we stopped Aspirin and continued Plavix only as a life-long medication. The patient's condition remained normal at 84 months.
DISCUSSION
Most of the information on isolated spontaneous dissections of the visceral arteries comes from sporadic case reports of single artery dissections, mostly involved the splanchnic artery [1256]. To the best of our knowledge, this is the first report on multiple simultaneous visceral artery dissections which have endured the longest follow-up without event (84 months). Management of this condition is usually challenging because this is a dynamic process and its evolution over time is completely unknown since spontaneous resolution, definitive occlusion of the visceral artery, aneurysm formation, or rupture are all possible [7]. Moreover, there has been no consensus on therapeutic strategy and the approach employed is often case by case. Medical treatment and regular imaging surveillance are generally recommended for uncomplicated asymptomatic dissections. Administration of anticoagulation or antiplatelet agents for 3 to 6 months with a target international normalized ratio of 2.0 to 3.0 has been suggested to prevent thromboembolic complications [568]. Initially, we treated conservatively as suggested in the literature [15689]. However, bowel ischemia was strongly suspected thereafter because of persistent abdominal pain and diffuse tenderness even though CT findings were inconclusive. In addition, the patient had both SMA and CA dissections which may have compromised the blood flow to multiple affected organs. Therefore, we believed that SMA stenting, rather than conservative treatment alone, to improve the splanchnic perfusion and prevent further complication was essential. Conversely, a CA dissection is usually nonfatal in nature and less associated with organ ischemia than that of the SMA because of the abundant blood supply from the SMA. Once the SMA is sufficiently reperfused, flow to the CA improves. Therefore, a CA dissection would rarely lead to any serious sequelae when the dissection is limited to the celiac trunk in the acute or early phase [10]. Increased serum creatinine, leukocytosis and markedly increased levels of serum LDH and evidence of renal infarction on the CT were consistent with renal parenchymal cell death [3]. Thus, we considered revascularization to promptly improve perfusion and to prevent renovascular hypertension afterward. After SMA and left renal artery stenting, the patient was free of pain with normalized laboratory results and blood pressure.
In this case, the etiology of multiple dissections was unclear except for several underlying risk factors such as alcohol consumption, being male and of middle age. Shearing stress, arterial dysplasia and vasa vasorum abnormalities have been viewed as predisposing factors for spontaneous peripheral arterial dissections, however, the natural history, etiology and exact incidence of this condition remain unclear [12569]. The prognosis of visceral artery dissection used to be poor. However, its outcome has improved significantly due to the advancements of conservative treatments, surgical techniques and endovascular interventions [248].
In conclusion, we reported an extremely rare case of spontaneous dissections of multiple visceral arteries in a healthy man. The patient has the longest follow-up duration without event. In spite of controversial treatment strategies and unclear long-term outcomes of this condition, percutaneous endovascular intervention is technically feasible, effective and reliable.

 XML Download
XML Download