

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Colonic anastomosis is one of the major prodecures of both elective and urgent general surgical procedures. When a complication occurs due to a colonic anastomosis, morbidity and mortality become an important issue [1]. In the general health status of the patient, whether the anastomosis is elective or emergent, preoperative preparation and surgical technique are parts of a successful colonic anastomosis. Although many advances have been accomplished in colonic anastomosis, the rate of leakage reaches 35% in some series [2].
Appropriate surgical technique is the mainstay of a successful surgical outcome. Nowadays, using electrosurgical devices is an inseparable part of daily surgical practice. Not only has monopolar electrocautery become one of the fixtures of the operating theatre but vessel sealing bipolar electrocurgical devices have also become a fixture of the operating theatre.
Although using such devices have shortened operating time and have prevented blood loss, tissue damage created by electrical energy has been a drawback for the use of electrosurgical equipment for special anatomic features where adequate blood flow is mandatory for healing. Blood flow and minimal tissue damage in colonic anastomosis are crucial for a successful anastomosis [3].
In this experimental study, the effect of bowel transsection technique on colonic anastomotic healing is investigated.
The effect of resection with scalpel, monopolar cautery and harmonic scalpel on colonic anastomotic healing are compared.
METHODS
The study was conducted in the Experimental Laboratories of Ankara Education and Research Hospital after ethical consent was granted by the local ethical committees (28.01.2011/19). One hundred twenty female Wistar Albino rats each weighing 220–240 g were used in the study. The rats were kept under a temperature of 20℃–25℃, humidity of 40%, and 12 hours of daylight. They were fed with rat chow of 2700 ME kcal/kg and 24% HP in pellet form and they had free access to water.
Animals were divided into 3 groups each consisting of 40 rats. They were weighed before surgery and before sacrification to identify any weight loss. The rat chow consumed before surgical procedure and after sacrification were weighed in order to assess the well being of the animals.
Rats were not given rat chow 12 hours prior to surgery but had free access to water until the time of operation.
Study groups were as follows:
Group A: colon resection by scalpel (40 rats) (group A1, sacrification on 1st postoperative day [10 rats]; group A3, sacrification on 3rd postoperative day [10 rats]; group A5, sacrification on 5th postoperative day [10 rats]; group A7, sacrification on 7th postoperative day [10 rats])
Group B: colon resection by monopolar electrocautery (group B1: Sacrification on 1st postoperative day [10 rats]; group B3: Sacrification on 3rd postoperative day [10 rats]; group B5: Sacrification on 5th postoperative day [10 rats]; group B7: Sacrification on 7th postoperative day [10 rats])
Group C: colon resection by harmonic scalpel (group C1: Sacrification on 1st postoperative day [10 rats]; group C3: Sacrification on 3rd postoperative day [10 rats]; group C5: Sacrification on 5th postoperative day (10 rats); group C7: Sacrification on 7th postoperative day [10 rats])
All of the groups were subdivided into 4 groups each consisting of 10 rats, as the rats were sacrificed on the 1st, 3rd, 5th, and 7th days postoperatively.
General anesthesia was induced by intraperitoneal ketamin 90 mg/kg (Ketalar, 500 mg/10 mL Pfizer, Berlin, Germany) xylazine 10 mg/kg (Rompun, Bayer, Leverkusen, Germany). A midline laparotomy was accomplished after the abdomen was shaved and cleaned with povidone iodine. Distal colon was prepared for surgery.
Surgical intervention: In group A, a colonic resection of 5 cm distal to the ileoceacal valve was accomplished by scalpel, in group B by monopolar electrocautery (coagulation mode, 60 W, Martin ME 411, Gebrüder Martin GmbH & Co. KG,, Tuttlingen, Germany) and in group C by harmonic scalpel (level 3, Ethicon Inc., Somerville, NJ, USA). The cut ends of the colon were anastomosed by 8–12 interrupted inverting sutures of taper point 6/0 polypropylene suture. In order to exclude the unwanted effects of both suture material and anastomotic suture techniques, single-layer interrupted 6/0 polypropylene and inverting suture techniques were preferred. Peritoneum and fascia were closed by interrupted 3/0 polypropylene suture and skin was closed by interrupted 3/0 silk suture.
The rats were allowed to feed on postoperative day 1 with rat chow and water. Rats were sacrificed on 1st, 3rd, 5th, and 7th postoperative days according to their groups by high-dose ketamine administration.
The abdomen was opened via the old incision. The anostomosis was observed macroscopically and changes were noted. The anastomotic line was taken as a sample for histopathologic examination in 5 rats from each subgroup without rendering the anastomosis and were put into 10% formaline. In all rats, apart form these five rats in each group and rats in groups A1, A3, B1, B3, C1, C3; bursting pressures were measured in situ without dissecting any adhesions. After this measurement, colon tissue samples were taken including tissue 1 cm distal and proximal to the anastomotic line for biochemical and histopathological analysis.
Measurement of bursting pressure
The bursting pressure of the colonic anastomosis was measured in situ using an infusion pump and a manometer. The colon was closed with 3/0 silk suture 2 cm distal to the anastomosis and was cut 2 cm proximal to the anastomosis. The anastomotic sutures were left in place. The fecal content in the colonic segment was washed with saline and a catheter connected to the infusion pump was secured in an air tight manner to the cut end of the colon. The abdomen was filled with water and the anastomotic segment was kept under water level. Two milliliters per minute air was sent at a constant rate into the segment and the anastomotic segment was inspected closely. The pressure at which air bubbles appeared around the anastomotic line was noted as bursting pressure.
Measurement of tissue hydroxyproline in perianastomotic tissues
As hydroxyproline constitutes one third of the amino acids in collagen, the measurement of tissue hydroxyproline was taken as a surrogate parameter for estimating the collagen content in perianastomotic tissues. Tissue hydroxyproline measurement is based on the spectrophotometric measurement of chromogen complex at 560 nm formed by the reaction between 4-hyroxyproline and chloramine-T (Na chloro-p-toluen sulphonamide). Hydroxyproline is oxidized to pyrole or pyrole-2-carboxylic acid and interacts with Ehrlich's reagent to form the chromogen complex.
After anastomotic bursting pressure was measured, a 1-cm colonic segment including both sides of the anastomosis was resected and washed with saline to be kept at –80℃.
After thawing, all of the specimens were weighed and 100 mg of tissue was put in a test tube and 1 mL of 12 N HCl was added. Tissue samples were hydrolyzed by keeping the tubes for one hour at 150℃ in dry air oven. Ten microliter of hydrolyzed tissue was taken and put into new test tubes and were left to dry for 24 hours. At the end of the drying process, 0.2 mL of chloramine-T solution was added and after 10 minutes, 1 mL of Ehrlich's reagent was added to the tube and stirred. Test tubes were kept at 50℃ for 90 minutes. Afterwards, the tubes were cooled under tap water for 2–3 minutes and absorbance of Ehrlich's reagent was read at 560 nm by spectrophotometry.
Histopathologic examination
Paraffin blocks were prepared from tissue samples that were kept in 10% formaline. Five-micron-thick slices were prepared and painted by haematoxyline eosine. The samples were examined by a blinded pathologist under light microscopy (U-MDOB3, Olympus, Tokyo, Japan).
Statistical analysis
SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Shapiro-Wilk test was used to see whether the continous variables had a normal distrubition. For descriptive statistics, mean ± standard deviation was used for hydroxyproline levels and bursting pressure and median (range) was used for histopathologic parameters. The significance of difference for hydroxyproline levels and bursting pressure among the groups was tested by one-way analysis of variance. If a statistically significant difference was observed, the reason for this difference was sought using post hoc Tukey test. Kruskall-Wallis test was used to detect any statistically significant difference among the groups for histopathological parameters. If a significant difference was found, Mann-Whitney U-test was used to search for the difference between the groups. A P-value of <0.05 was taken as statistically signficant and confidence interval was 95%. In order to control possible type 1 error in all of the multiple comparisons, Bonferroni correction was applied.
RESULTS
Six rats were lost during the study, 4 from group B and 2 from group C. The rats were replaced by new rats. Necropsies of the dead animals revealed severe peritonitis due to macroscopic anastomotic leakage.
The authors observed that colon resection done by scalpel and subsequent anastomosis were more difficult because of bleeding, although no animal was lost. Electrocautery provided a very suitable surgical field for anastomosis. Harmonic scalpel also provided a very suitable surgical field without bleeding but as the cut ends of the colon were closed during the procedure, opening the obliterated ends was time consuming.
Physical parameters of the rats
Though statistically insignificant, the weight measurement of the rats in group A were higher than other groups on the 1st, 3rd, and 5th days of the experiment. On day 7, there was no difference for weight measurement in any of the groups.
Bursting pressure
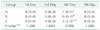
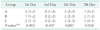
On the 5th day, the highest mean bursting pressure was observed in group A (170 ± 17.32 mmHg) while mean bursting pressure values were lower in group B (84 ± 35.78 mmHg), with the lowest mean pressure observed in group C (74 ± 29.66 mmHg). There was a statistically significant difference between group A and both group B and group C (P < 0,001). There was no statistically significant difference between groups B and C (P = 0.781).
On the 7th day, mean bursting pressures for groups A, B, and C were 226 ± 59.41, 180 ± 14.14, and 213 ± 54.04 mmHg, respectively, without any significant difference among the groups (P = 0.182).
The values for bursting pressures on the 5th and 7th day are given in Table 5.
Hydroxyproline level measurement
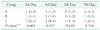
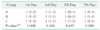
There was no statistically significant difference among the groups for hydroxyproline levels in anastomotic tissue on the 1st, 3rd, 5th, and 7th days (P = 0.059, P = 0.318, P = 0.093, P = 0.472, respectively). Hydroxyproline levels are given in Table 6.
Histopathologic examination
Histologic changes induced by anastomotic healing, granulation tissue formation and local inflammatory reaction were evaluated according to parameters modified by Parra-Membrives et al. [4].
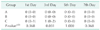
There was no statistically significant difference for mucosal reepithelization in all groups for all of the study days (P = 0.257, P = 0.116, P = 0.030, P = 0.031) (Table 7).
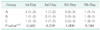
No analysis could be performed for no inflammatory cell reaction could be detected microscopically. No statistically significant difference could be found for neovascularization among the groups (P = 0.422) (Table 8).
On the 5th postoperative day, fibroblast proliferation and fibrosis were significantly higher in group C when compared to groups A and B (P = 0.006, P = 0.006). No significant difference could be found for other groups (Tables 9, 10).
There was no stastically signficant difference between study groups when compared for ischemic necrosis at muscularis mucosa (P = 0.803, P = 0.247, P = 0.459, P = 0.136) (Table 11).
There was no stastically signficant difference between study groups when compared for completeness of muscle tissue (P = 0.368, P = 0.031, P = 1.000, P = 0.368) (Table 12). There was no stastically signficant difference between study groups when compared for inflammation (P = 0.500 P = 0.259, P = 1.000, P = 0.584) (Table 13). There was no stastically signficant difference between study groups when compared for neutrophil infiltration (P = 0.493, P = 0.497, P = 0.097, P = 0.038) (Table 14). There was no stastically signficant difference between study groups when compared for lymphocyte infiltration scores (P = 1.000, P = 0.584, P = 0.497, P = 0.280) (Table 15).
No statistical evaluation could be done for giant cells and monocytes as they could not be detected in pathology specimens.
DISCUSSION
Intestinal anastomosis is one of the principle surgical procedures in gastrointestinal surgery that can have high mortality and morbidity rates when anastomotic leakage or dehiscence occur [5]. These complications are more common (13%–69%) in colonic anastomoses due to various factors like high collagenase activity, decreased collagen content, impaired collateral circulation and absence of serosa in distal rectum [6].
Decreasing the complication rate in gastrointestinal anastomosis has always been an important research topic. Different surgical techniques for anastomosis, pharmocologic agents, suture materials have not overcome the problem completely [7].
Scalpel dissection is the standard way of dissecting tissues. Despite being economic and easy to use, the lack of hemostasis leading to time loss during surgery, the need for hemostatic sutures that act as foreign material, and risk of inadvertent injuries to the surgical team are the main disadvantages [8].
Electrocautery, invented at the beginning of the 20th century, has overcome these disadvantages of scalpel [9]. This type of electrosurgery uses heat energy to denature proteins to ensure hemostasis [10]. The main disadvantage of electrocautery is tissue damage created by heat energy [11]. Clinical studies have shown that wound healing can be imparied and the patient's healing process can be complicated with severe postoperative pain and weight loss [12].
Harmonic scalpel is one of the latest devices of electrosurgery. In this technology, mechanical energy is converted to ultrasonic energy via piazo electric crystals. This resultant minimal energy breaks hydrogen bonds and induces hemostasis by protein denaturation.
Scalpel is favored over electrocautery for skin, subcutaneous tissue and fascia incisions [13], as there are studies which state that scalpel incisions have less wound infections and an increased wound strength [14]. There are studies which state the opposite stating there is no difference for wound infection for scalpel and electrocautery [15].
Anastomotic wound healing can be assessed by histolopathologic, biochemical, and mechanical means [16]. Histopathologic examination is the assessment of the phases of wound healing of the anastomosis [17]. The aim of anastomotic healing is to restore tissue strength to levels before the anastomosis [18], and this depends upon the quality and the quantity of the newly synthetized collagen [19]. Biochemical examination is the measurement of hydroxyproline content of the anastomosis as a surrogate parameter of collagen synthesis [20]. Mechanical examination is the bursting pressure of the anastomosis [21].
Examination of anastomotic healing in this study was scheduled for the 1st, 3rd, 5th, and 7th days. The first day was chosen to denote early changes. The third day was chosen as collagenase activity is maximal on this day. The 5th and 7th days were chosen as it is known that bursting pressures increase after the 5th day and on the 7th day increased anastomotic strength is more evident [22].
The tissue HP levels did not show any significant difference between the groups and subgroups. The mean bursting pressure of the group A on the 5th day was significantly higher than groups B and C (P < 0.001). No mortality was observed in this group and feeding parameters were much better, which supports the general well being of the subjects. When the fibroblast and fibrosis scores were evaluated scores of the group C on the 5th day were significantly higher than the other groups, but the results of bursting pressures and biochemical parameters did not support the fibroblast and fibrosis scores. There were not any significant difference between the groups about other histopathologic parameters on any day. The mortalities observed in the early phases of the experiment suggest that monopolar cautery should be used with caution as the tissue damage can lead to disruption of the anastomosis where the equilibrium between hemostasis and intestinal blood flow is delicate. Although it provides hemostasis without major tissue damage, the obliterative property of harmonic scalpel interferes with its use.
Significantly higher bursting pressures observed on the 5th day, higher bursting pressures on 7th day (although not significant), observation of no mortality, and better chow consumption in group A brought us to the conclusion that although it is time consuming and difficult to create an anastomosis because of bleeding, resection using scalpel is much better for the integrity of colonic anastomosis due to minimal tissue damage, obliteration of dead spaces, and reduction of ischemic and necrotic tissue. This result should be supported by large clinical series.





 XML Download
XML Download