

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Atopic dermatitis is one of the most common allergic diseases, and its prevalence has been increasing in recent decades. Social economic status is a well-known risk factor for allergic disease. This study was performed to investigate the relationship between social economic status and atopic dermatitis in Korean adults.
Methods
Data were acquired from 18,066 men and women aged older than 19 years who participated in the Fifth Korea National Health and Nutrition Examination Surveys (KNHANES), which was conducted from 2010 to 2012. The presence of atopic dermatitis was based on self-reported physician diagnosis of atopic dermatitis in the Health Interview Surveys.
Results
The prevalence of atopic dermatitis was 2.3%, which decreased with age. In univariate analysis, adults with atopic dermatitis were younger, well-educated, had higher monthly family income, had more household members, and lived in the urban area (P<0.05), whereas sex, residential type, or smoking status was not associated with the presence of atopic dermatitis. The prevalence of hypertension, diabetes mellitus, and obesity were lower in atopic dermatitis subjects, while asthma was higher (P<0.05). Binary logistic regression analysis showed that younger age and the presence of asthma were associated with higher prevalence of atopic dermatitis (P<0.01).
Conclusion
The results of this study suggest that younger age and the prevalence of asthma may be important risk factors for the prevalence of atopic dermatitis in Korean adults. These results warrant future studies to explore mechanisms underlying the association between social economic status and atopic dermatitis.
Figures and Tables
Table 1
Demographic characteristics of subjects (n=18,066)

Table 2
Atopic dermatitis prevalence among adults in Korea, The Fifth Korea National Health and Nutrition Examination Survey (2010-2012)
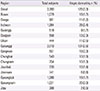
Table 3
Demographic characteristics according to the presence of atopic dermatitis (n=18,066)

Table 4
Comorbidity conditions in atopic dermatitis subjects (n=18,066)

Table 5
Adjusted odd ratio (OR) and their 95% confidence interval (CI) for the prevalence of atopic dermatitis

References
1. Williams H, Flohr C. How epidemiology has challenged 3 prevailing concepts about atopic dermatitis. J Allergy Clin Immunol. 2006; 118:209–213.

2. Hong SJ, Lee MS, Sohn MH, Shim JY, Han YS, Park KS, et al. Self-reported prevalence and risk factors of asthma among Korean adolescents: 5-year follow-up study, 1995-2000. Clin Exp Allergy. 2004; 34:1556–1562.
3. Lee SI, Shin MH, Lee HB, Lee JS, Son BK, Koh YY, et al. Prevalences of symptoms of asthma and other allergic diseases in korean children: a nationwide questionnaire survey. J Korean Med Sci. 2001; 16:155–164.
4. Williams H, Stewart A, von Mutius E, Cookson W, Anderson HR. International Study of Asthma and Allergies in Childhood (ISAAC) Phase One and Three Study Groups. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008; 121:947–954.e15.
5. Muto T, Hsieh SD, Sakurai Y, Yoshinaga H, Suto H, Okumura K, et al. Prevalence of atopic dermatitis in Japanese adults. Br J Dermatol. 2003; 148:117–121.
6. Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013; 132:1132–1138.
7. Kim MJ, Kang TW, Cho EA, Kim HS, Min JA, Park H, et al. Prevalence of atopic dermatitis among Korean adults visiting health service center of the Catholic Medical Center in Seoul Metropolitan Area, Korea. J Korean Med Sci. 2010; 25:1828–1830.
8. Hammer-Helmich L, Linneberg A, Thomsen SF, Glumer C. Association between parental socioeconomic position and prevalence of asthma, atopic eczema and hay fever in children. Scand J Public Health. 2014; 42:120–127.
9. Hunter JA, Herd RM. Recent advances in atopic dermatitis. Q J Med. 1994; 87:323–327.
10. Nishioka K. Atopic eczema of adult type in Japan. Australas J Dermatol. 1996; 37:Suppl 1. S7–S9.
11. Saeki H, Tsunemi Y, Fujita H, Kagami S, Sasaki K, Ohmatsu H, et al. Prevalence of atopic dermatitis determined by clinical examination in Japanese adults. J Dermatol. 2006; 33:817–819.
12. Harrop J, Chinn S, Verlato G, Olivieri M, Norback D, Wjst M, et al. Eczema, atopy and allergen exposure in adults: a population-based study. Clin Exp Allergy. 2007; 37:526–535.
13. Hanifin JM, Reed ML. Eczema Prevalence and Impact Working Group. A population-based survey of eczema prevalence in the United States. Dermatitis. 2007; 18:82–91.
14. Ring J, Kramer U, Schafer T, Abeck D, Vieluf D, Behrendt H. Environmental risk factors for respiratory and skin atopy: results from epidemiological studies in former East and West Germany. Int Arch Allergy Immunol. 1999; 118:403–407.
15. Xu F, Yan S, Li F, Cai M, Chai W, Wu M, et al. Prevalence of childhood atopic dermatitis: an urban and rural community-based study in Shanghai, China. PLoS One. 2012; 7:e36174.
16. Keil T, Lau S, Roll S, Gruber C, Nickel R, Niggemann B, et al. Maternal smoking increases risk of allergic sensitization and wheezing only in children with allergic predisposition: longitudinal analysis from birth to 10 years. Allergy. 2009; 64:445–451.
17. Schafer T, Dirschedl P, Kunz B, Ring J, Uberla K. Maternal smoking during pregnancy and lactation increases the risk for atopic eczema in the offspring. J Am Acad Dermatol. 1997; 36:550–556.
18. Miyake Y, Miyamoto S, Ohya Y, Sasaki S, Matsunaga I, Yoshida T, et al. Association of active and passive smoking with allergic disorders in pregnant Japanese women: baseline data from the Osaka Maternal and Child Health Study. Ann Allergy Asthma Immunol. 2005; 94:644–651.
19. Oryszczyn MP, Annesi-Maesano I, Charpin D, Paty E, Maccario J, Kauffmann F. Relationships of active and passive smoking to total IgE in adults of the Epidemiological Study of the Genetics and Environment of Asthma, Bronchial Hyperresponsiveness, and Atopy (EGEA). Am J Respir Crit Care Med. 2000; 161(4 Pt 1):1241–1246.
20. Lee CH, Chuang HY, Hong CH, Huang SK, Chang YC, Ko YC, et al. Lifetime exposure to cigarette smoking and the development of adult-onset atopic dermatitis. Br J Dermatol. 2011; 164:483–489.
21. Pourpak Z, Mozaffari H, Gharagozlou M, Daneshmandi Z, Moin M. Asthma in patients with atopic dermatitis. Indian J Pediatr. 2008; 75:139–141.
22. Beuther DA, Weiss ST, Sutherland ER. Obesity and asthma. Am J Respir Crit Care Med. 2006; 174:112–119.
23. Ford ES. The epidemiology of obesity and asthma. J Allergy Clin Immunol. 2005; 115:897–909.
24. Shore SA, Johnston RA. Obesity and asthma. Pharmacol Ther. 2006; 110:83–102.
25. Kilpelainen M, Terho EO, Helenius H, Koskenvuo M. Body mass index and physical activity in relation to asthma and atopic diseases in young adults. Respir Med. 2006; 100:1518–1525.
26. Uehara M, Ofuji S. Abnormal vascular reactions in atopic dermatitis. Arch Dermatol. 1977; 113:627–629.
27. Uehara M, Sugiura H, Tanaka K. Rarity of hypertension in adult patients with atopic dermatitis. Br J Dermatol. 2002; 146:631–635.
28. Olesen AB, Juul S, Birkebaek N, Thestrup-Pedersen K. Association between atopic dermatitis and insulin-dependent diabetes mellitus: a case-control study. Lancet. 2001; 357:1749–1752.
29. Agrawal R, Wisniewski JA, Woodfolk JA. The role of regulatory T cells in atopic dermatitis. Curr Probl Dermatol. 2011; 41:112–124.
30. Lan RY, Ansari AA, Lian ZX, Gershwin ME. Regulatory T cells: development, function and role in autoimmunity. Autoimmun Rev. 2005; 4:351–363.
 XML Download
XML Download