

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cough is intrinsically a protective reflex, but becomes troublesome when hypersensitive and persistent. Chronic cough is a prevalent problem in about 10% of the general populations worldwide.1 The prevalence is lower in Asians than in Western populations,1 but the burden of chronic cough will continue to increase in Asian countries as the prevalence is positively associated with Westernized lifestyles and old age.23 Meanwhile, chronic cough poses a considerable socioeconomic burden and serious impairment to quality of life (QOL).4567 Patients with chronic cough may experience physical pain, sleep disturbance, loss of work productivity, and social isolation for several months to years.5689
Patients visiting clinics for the treatment of chronic cough commonly complain of unexpected cough attacks triggered by trivial stimuli, such as cold air, perfume, or talking, which are not relevant to the intrinsic roles of the cough reflex.10 Along with recent advances in understanding the pathology of chronic cough, a new paradigm, “Cough Hypersensitivity Syndrome,” was recently proposed by the European Respiratory Society (ERS) to emphasize the clinical relevance of the intrinsic neurological processes in chronic cough.1112 Several factors may underlie this “chronic cough hypersensitivity,” but several pathological conditions located at sensory nerve endings that regulate the cough reflex, such as rhinitis, rhinosinusitis, asthma, eosinophilic bronchitis, and gastroesophageal reflux diseases (GERDs), are considered to be particularly important.13 Therefore, identification and treatment of these conditions, termed as “anatomic diagnostic protocols,” are the mainstay of current international clinical practice guidelines for the treatment of chronic cough.1415 However, the epidemiology of these comorbid (or cough-triggering) conditions, healthcare accessibility, and medical issues may vary among regions and populations, which is a main reason to develop region-specific clinical practice recommendations and guidelines.16
Chronic cough is frequently non-specific and accompanied by not easily identifiable causes during the initial evaluation. However, objective diagnostic tools for the most common conditions, such as asthma, eosinophilic bronchitis, and GERD, are technically demanding and not available in most general clinics. Indeed, the focus of most previous guidelines has been secondary or tertiary care settings.16 Therefore, there are major unmet needs for empirical treatment and practical diagnostic approaches that can be applied in primary clinics for the treatment of chronic cough.
Meanwhile, in referral clinics, there is increasing recognition that a considerable proportion of adult patients are refractory to conventional treatment and do not fit into any categories despite meticulous diagnostic and therapeutic trials.11 This subgroup has been termed as refractory, idiopathic, or unexplained cough, while the term “unexplained chronic cough” has recently been suggested by the American College of Chest Physician (ACCP) guidelines.17 However, management tools for this particular population are not established.
Definition of chronic cough
Chronic cough is defined as cough lasting more than 8 weeks in adults (aged ≥ 15 years old) and more than 4 weeks in children (aged < 15 years old).
Non-specific chronic cough indicates prolonged cough in the absence of any symptoms, signs, history, or laboratory findings indicating a specific diagnosis for chronic cough (specific cough pointers): current use of angiotensin-converting enzyme inhibitors (ACEi), current smoker, any evident symptoms indicating a specific diagnosis, such as fever, blood-tinged sputum, wheezing, dyspnea, rhinorrhea, nasal obstruction, or heartburn, abnormal physical findings, such as wheezing or crackles on auscultation, or abnormal findings on chest X-rays and/or spirometry.
Chronic wet cough is defined as cough accompanied by airway secretion, which is unrelated to any specific cough pointers in children.
Unexplained chronic cough refers to cough with an unknown etiology after thorough investigation and therapeutic trials conducted according to current practice guidelines.17 The investigation and therapeutic trials should include those for common cough-triggering conditions (rhinitis, rhinosinusitis, asthma, eosinophilic bronchitis, and GERD) and might include computed tomography or bronchoscopy to exclude rare causes which are not identified on chest X-rays (Table 1 and Fig. 1).
Table 1
Definition of chronic cough utilized in the present clinical practice guidelines
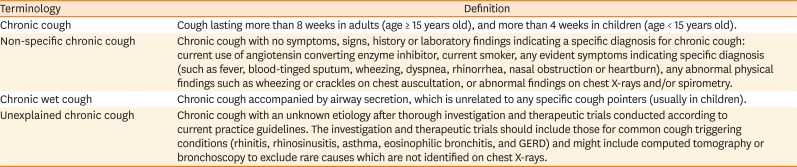
Fig. 1
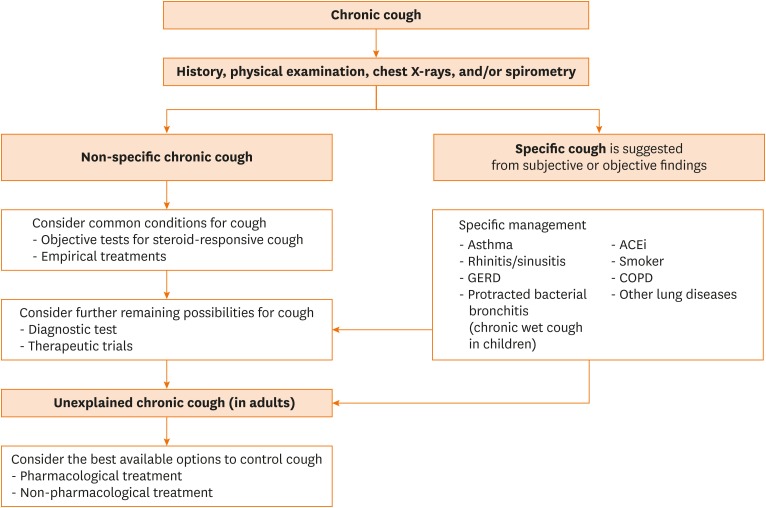
Overview of clinical approaches for the treatment of chronic cough in Korean patients.
The initial investigation includes a comprehensive medical history, physical examination, chest X-rays, and/or spirometry (when available). If the cough is non-specific, objective tests for steroid-responsive cough and empirical trials are recommended. When clues suggest specific cough conditions, specific management should be followed. If cough remains unexplained after thorough investigation and therapeutic trials in adults, further pharmacological and non-pharmacological options are recommended to control cough.
ACEi, angiotensin converting enzyme inhibitors; GERD, gastroesophageal reflux disease; COPD, chronic obstructive pulmonary disease.
Unmet patient needs
A recent survey of Korean patients with chronic cough (n = 402) (manuscript in preparation) found that the most common dissatisfaction with medical cares for cough was the lack of treatment efficacy (50.0%), followed by the lack of a specific diagnosis (29.3%). About 85% of the patients surveyed found it difficult to identify cough specialists and clinics, and about two-thirds had tried over-the-counter medicines for cough, but only 2.8% reported effective symptom relief.
Scope of guidelines
The present clinical practice guidelines aim to address major clinical questions regarding empirical treatment, practical diagnostic tools for non-specific chronic cough, and available therapeutic options for chronic wet cough in children and unexplained chronic cough in adults. Meanwhile, management of specific cough conditions (such as asthma or reflux-associated cough) is beyond the scope of the present guidelines.
MATERIALS AND METHODS
Methodology specialist coordinated and guided committee members throughout the entire process of conducting systematic reviews, generating recommendations, and ensuring methodological robustness, according to the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.18 The members of the guideline development committee participated in literature searches, data extraction, evidence synthesis, and formulating recommendations. All members were required to disclose any potential conflicts of interest.
Formulating questions
The committee members consisted of clinicians with different specialties (allergy, pulmonology, internal medicine, pediatrics, rhinology, and family medicine) and clinical settings (referral hospitals and primary clinics) who participated in discussions and arrived at a consensus to formulate key clinical questions that would be addressed in the guidelines. The findings from the questionnaire survey about unmet patient needs when seeking medical care for chronic cough were also considered (manuscript in preparation). Through this process, the committee members formulated a list of key questions that are important for the diagnosis and treatment of chronic cough in Korea. The population, intervention, comparison, and outcomes (PICO) format were used to construct the questions.
Literature searches
The MEDLINE, Embase, Cochrane Central Register of Controlled Trials, Scopus, Web of Science, and KoreaMed databases were searched for relevant articles from inception until June 28, 2016. Manual searches were performed for cross-referenced articles. Also, unpublished randomized controlled trials (RCTs) were retrieved from the ClinicalTrials.gov database. There was no language restriction.
Study selection
The relevancy of the retrieved studies was confirmed by at least 2 independent reviewers per each PICO question, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Briefly, the titles and abstracts of initially retrieved studies were screened and the full texts were reviewed for potentially relevant papers. Reasons for exclusion were specified. Disagreements between reviewers were resolved by discussion and consensus within the committee.
Risk of bias assessment
Risks of bias were assessed using the Cochrane Collaboration's risk of bias tool (for RCTs), the Newcastle-Ottawa quality assessment scale (for cohort or case-control studies), and the QUADAS-2 tool (for diagnostic accuracy studies). Disagreements between reviewers were resolved by discussion and consensus within the committee.
Evidence synthesis
Data regarding baseline characteristics and core outcomes of each PICO question were extracted for analysis. The Mantel-Haenszel method or the inverse variance method with a random effects model was used to summarize treatment efficacy and/or safety. A random effects hierarchical summary receiver operating characteristic model was used to calculate diagnostic test properties. The meta-analysis was performed using RevMan software for preparing and maintaining Cochrane Reviews (version 5.3; the Nordic Cochrane Centre, Copenhagen, Denmark) and STATA statistical software (version 13.1; Stata LLC, College Station, TX, USA). The GRADEpro Guideline Development Tool (McMaster University, Hamilton, ON, Canada) was used to summarize evidence profiles for each outcome.
Grading quality of evidence and strength of recommendations
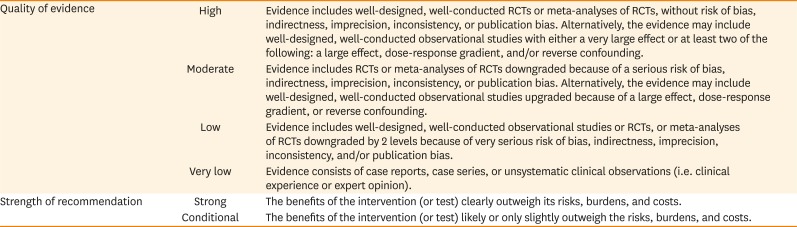
The quality of evidence was rated for outcomes of interest (efficacy and safety of treatment agents, and diagnostic accuracy and safety of diagnostic tests) for each PICO question according to the GRADE approach.18 Briefly, the evidence supported by RCTs was considered high quality, while that of observational studies as low quality. Five factors were considered for possible down-rating of a study (risk of bias, inconsistency, indirectness, imprecision, and publication bias) and 3 factors for possible up-rating (large effects, dose response, and all plausible residual confounders). Then, the committee members determined the direction and strength of recommendations based on the following considerations: balance of benefits and undesirable consequences of intervention (or diagnostic test), quality of evidence, patient values and preferences, and feasibility.
Briefly, one of 2 grades (strong or conditional) were assigned to describe the strength of recommendations. The criterion for a strong recommendation was evidence that the desirable effects clearly outweighed the undesirable effects (or vice versa). The criterion for a conditional recommendation was evidence that the desirable effects likely or slightly outweighed the undesirable effects (or vice versa). Two classifications were used to indicate the direction of recommendations (for or against) of a specific treatment or test (Table 2).
Table 2
Classification for quality of evidence and strength of recommendation in the present guidelines
The recommendations generated by the committee were then sent for a public hearing, where an agreement on the criteria was more than 70% of votes in favor. If no agreement was reached, the PICO question was further discussed by the committee for possible adjustment of the recommendation.
KEY QUESTIONS
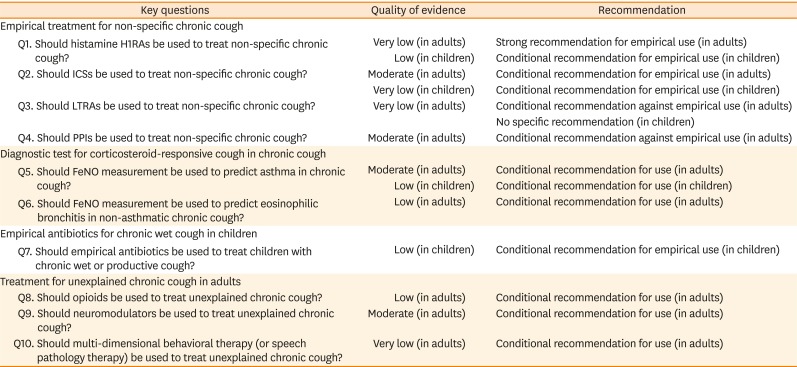
Responses to the following 10 questions were used to assess systematic reviews retrieved from the literature to generate recommendations with the GRADE approach (Table 3).
Table 3
Summary of key questions and recommendations
I. Empirical treatment for non-specific chronic cough
Q1. Should histamine H1-receptor antagonists (H1RAs) be used to treat non-specific chronic cough? (in both adults and children)
Q2. Should inhaled corticosteroids (ICSs) be used to treat non-specific chronic cough? (in both adults and children)
Q3. Should leukotriene receptor antagonists (LTRAs) be used to treat non-specific chronic cough? (in both adults and children)
Q4. Should proton pump inhibitors (PPIs) be used to treat non-specific chronic cough? (in adults)
I. EMPIRICAL TREATMENT FOR NON-SPECIFIC CHRONIC COUGH
Background
Upper airway diseases (rhinitis and rhinosinusitis), lower airway allergic inflammation (asthma and eosinophilic bronchitis), and GERD are well known as causes or triggers of chronic cough.15 These diseases are located close to the sensory endings of the vagus nerves, which regulate the cough reflex,13 thus diagnosis and treatment may improve cough in a considerable proportion of patients. Therefore, several medications with proven efficacy to control these diseases (i.e., histamine-1 receptor antagonists [H1RAs], inhaled corticosteroids [ICSs], leukotriene receptor antagonists [LTRAs], and proton-pump inhibitors [PPIs]) are commonly prescribed in current practice for the treatment of chronic cough, although none are direct anti-tussives.
Diagnosis of upper airway disease-related cough (termed as upper airway cough syndrome in the 2006 ACCP guidelines) is usually made clinically.14 To our knowledge, there is no predictor for the response of upper airway disease-related cough to H1RA treatment. Meanwhile, the diagnosis of corticosteroid-responsive cough conditions (asthma and eosinophilic bronchitis) can be made objectively by bronchial challenge or induced sputum testing. However, these tests are technically demanding and mostly unavailable in primary care settings. In addition, it is difficult to objectively discern causal and temporal relationships between acid reflux and cough in the majority of current clinical settings.19 Therefore, empirical treatment is frequently considered for non-specific chronic cough (Figs. 2 and 3). However, it is important to check whether patients have clues to specific cough conditions before starting empirical treatment. In particular, initial evaluation should include a comprehensive history, recent history of smoking and ACEi use, chest X-rays, and/or spirometry (if available) (Fig. 1).1415
Fig. 2
Approach for non-specific chronic cough in Korean adults (age ≥ 15 years).
Decision for empirical treatment and diagnostic tests may depend on clinical and instrument settings. Patients with chronic cough unresponsive to empirical trials or specific treatment should be referred to specialist centers for further diagnostic tests and therapeutic trials. If cough is still unexplained, pharmacological and non-pharmacological treatment options are considered to control cough.
H1RA, histamine-1 receptor antagonist; ICS, inhaled corticosteroid; PPI, proton-pump inhibitor; GERD, gastroesophageal reflux disease.
Asterisk (*) indicates the drug (or test) of interest in the present guidelines.
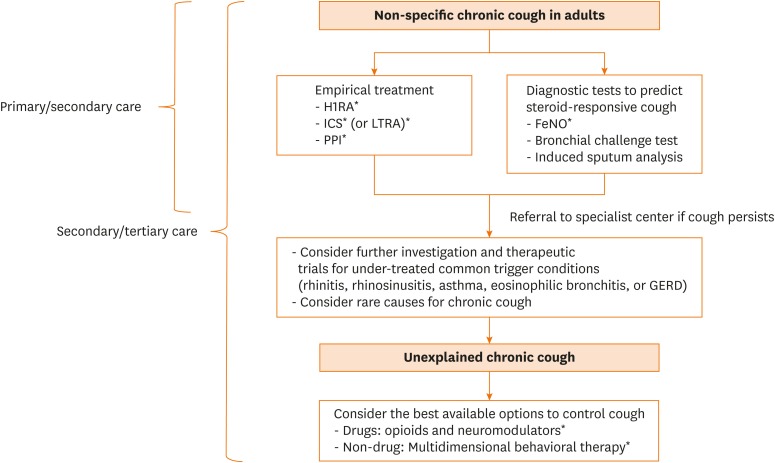
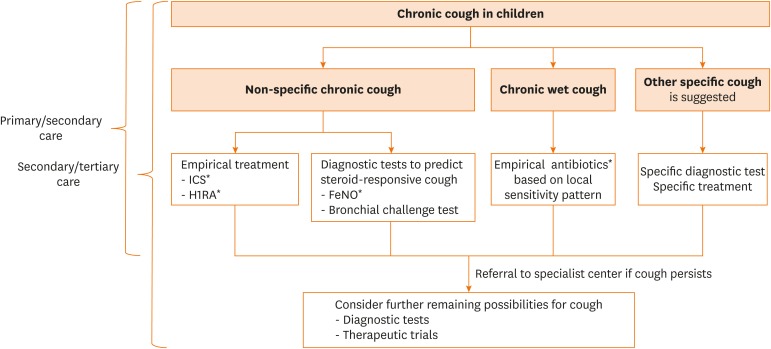
Fig. 3
Approach for non-specific chronic cough and chronic wet cough in Korean children (age < 15 years). Decision for empirical treatment and diagnostic tests may depend on clinical and instrument settings. Children with chronic cough unresponsive to empirical trials or specific treatment should be referred to specialist centers for further diagnostic tests and therapeutic trials.
ICS, inhaled corticosteroid; H1RA, histamine-1 receptor antagonist.
Asterisk (*) indicates the drug (or test) of interest in the present guidelines.
Q1. Should H1RAs be used to treat non-specific chronic cough? (in both adults and children)
Summary of evidence for adults
Three RCTs were identified.202122 Due to substantial differences in study designs and outcome definitions, a meta-analysis could not be conducted. However, all 3 RCTs found significant benefits from H1RA treatment as compared to placebos and negative controls. The outcomes were subjective cough frequency,20 distilled water-induced cough frequency,21 and cough severity score as measured from records recorded in a symptom diary.22 All were short-term clinical trials (treatment duration of <2 weeks) with older generation H1RAs (loratadine, diphenhydramine, or oxatomide).
Adverse effects from oral H1RAs are relatively well known and may include somnolence, dry mouth, dizziness, visual disturbance, motor disturbance, and/or voiding difficulty. Such adverse reactions are usually dose-dependent and self-limiting, and more prevalent with older generation H1RAs. Oral H1RAs are inexpensive and widely accessible in Korea.
Recommendation for adults
For adults with non-specific chronic cough, we recommend the empirical use of H1RAs (very low quality of evidence, strong recommendation). This recommendation is supported by the low costs, ease of accessibility, and tolerable safety profiles of H1RAs. However, possible side effects must be discussed with patients.
What others are saying for adults
For cases of suspected rhinitis-related cough or lacking a clear indication, the 2004 ERS guidelines recommended the empirical use of first-generation sedating H1RAs and/or oral decongestant for 2 weeks.15 However, these guidelines indicate that the site of action for sedating H1RAs is non-specific.15 The 2006 ACCP guidelines recommended the empirical use of first-generation H1RAs + oral decongestant combination for patients with non-specific chronic cough before proceeding to an extensive diagnostic workup.14
Summary of evidence for children
Two RCTs were identified.2324 The larger study randomly assigned 113 outpatients aged 6 to 26 months to receive either oral ketotifen (0.5 mg) or a placebo for 16 weeks. Cough was the major inclusion criterion, but children with wheeze were also included. Although there were no significant differences in clinical efficacy or adverse events between groups, the effect of the intervention could not be estimated as only 13 (11%) children had chronic cough alone.23 The smaller study randomly allocated 20 children, aged 6 to 15 years, with chronic cough associated with allergic rhinoconjunctivitis to daily cetirizine (0.15 mg/kg) or a placebo for 4 weeks. In this study, cough scores were significantly lower in the cetirizine group when compared to the placebo group, and the difference between the 2 arms was evident by week 2.24
Given the limitation of data specific to children with non-specific chronic cough, data could not be combined in a meta-analysis.
Recommendation for children
For children with non-specific chronic cough, we suggest against the empirical use of H1RAs (low quality of evidence, conditional recommendation). The use of H1RAs in children with non-specific cough must be balanced against the well-known adverse events, especially in very young children. Current data suggest that the use of H1RAs would be more efficacious in children with suspected allergic rhinitis.
What others are saying for children
The 2008 British Thoracic Society (BTS) guidelines recommended the empirical use of H1RAs in children with a throat clearing type of chronic cough and signs of allergic rhinitis.25 However, the 2017 ACCP guidelines recommended against the empirical use of H1RAs in children with chronic cough, unless other features consistent with upper airways cough syndrome due to rhinosinusitis are present.26
Q2. Should ICSs be used to treat non-specific chronic cough? (in both adults and children)
Summary of evidence for adults
Two randomized placebo-controlled trials were identified.2728 Both studies reported significant benefits in cough outcomes from a 2-week course of high-dose ICS treatment over placebo. Our meta-analysis found significant improvement in cough severity. Of note, the benefits were demonstrated with 2 weeks of starting treatment. In addition, the ICS treatment effects were correlated with type 2 airway inflammation biomarkers, such as FeNO levels.27 In a study of patients with non-asthmatic, non-eosinophilic chronic cough, which was not included in our systematic review, ICS treatment had no significant benefit over placebo.29 These discrepant findings indicate the mechanisms of action of ICSs.
Recommendation for adults
For adults with non-specific chronic cough, we suggest the empirical use of ICSs (moderate quality of evidence, conditional recommendation). Short-term (2-4 weeks), high-dose ICS treatment is recommended as an empirical regimen. Our guidelines suggest performing objective tests to diagnose asthma and eosinophilic bronchitis (such as methacholine challenge, induced sputum analyses, or FeNO measurement) prior to initiating empirical treatment where diagnostic tests are available because the documentation of corticosteroid-responsive conditions justifies long-term treatment. Otherwise, only short-term (2–4 weeks) treatment is warranted.
What others are saying for adults
The 2004 ERS guidelines recommended therapeutic trials starting with ICSs or oral prednisolone in patients without clues to specific cough-related conditions.15 Diagnostic tests may depend on clinical settings, but would include methacholine challenge tests and induced sputum tests to identify steroid-responsive cough. The 2006 ACCP guidelines recommended an empirical trial of corticosteroids in the absence of the availability of bronchial provocation tests and/or induced sputum analyses.14 Ideally, these tests are recommended before initiating corticosteroid therapy in patients with suspected cough due to asthma.
Summary of evidence for children
Our own systematic review identified one RCT of a total of 50 patients aged 1 to 10 years with non-specific chronic cough.30 The trial randomly assigned 50 outpatients with persistent nocturnal cough (more than 3 weeks) to receive either a placebo or fluticasone propionate at 1 mg twice daily for 3 nights and then 500 μg twice daily for 11 nights.
The main outcome measure was a decrease in cough frequency by 75% from baseline. Overall, symptoms improved by 75% after 2 weeks (P = 0.03) in 17 of 24 (71%) subjects who received inhaled corticosteroids and completed the study and 8 of 23 (35%) who received the placebo.
Recommendation for children
For children with non-specific chronic cough, we suggest the administration of ICSs for a well-defined period (very low quality of evidence, conditional recommendation). The use of high-dose ICSs in children with non-specific chronic cough must be balanced against well-known potential adverse events. A therapeutic trial of ICSs for young children with non-specific chronic cough is not ideal, but results from an imprecise definition of asthma and lack of available tests to confirm a diagnosis of asthma in young children. Before starting ICS therapy, therefore, a definite period of treatment (e.g., 2-4 weeks for high-dose ICS, and 8-12 weeks for conventional dose ICS) and objective end points should be set. If there is response and ICS treatment has subsequently been stopped, asthma is suggested by an early relapse that again responds to ICSs.
What others are saying for children
The 2008 BTS guidelines recommended a trial of ICSs or oral steroid with a definite period of time to diagnose problem coughing as being caused by asthma.25 The 2017 ACCP guidelines recommended empirical trial of ICS with a predefined time frame when the cough is dry and objective testing cannot be undertaken in a young child.26
Q3. Should LTRAs be used to treat non-specific chronic cough? (in both adults and children)
Summary of evidence for adults
Direct evidence of the efficacy of LTRAs for the treatment of non-specific chronic cough is lacking. No randomized placebo-controlled study was identified. One prospective observational study reported that montelukast therapy for 2 weeks significantly improved symptoms of chronic cough.31 However, the possibility of natural remission cannot be ruled out in an observational study lacking a control group. LTRAs were not effective in a RCT of 276 patients with subacute post-infectious cough, suggesting the lack of direct anti-tussive effects of LTRAs.32 Indirect evidence from small controlled trials of specific cough patient groups, such as cough variant asthma or eosinophilic bronchitis, suggested the potential benefits of LTRAs for the treatment of cough associated with asthma.333435
LTRAs are generally well-tolerated. However, our guideline panel had a concern about possible overuse of LTRAs for non-specific chronic cough, particularly in relation to the absence of direct evidence and lack of information on an optimal treatment duration.
Recommendation for adults
For adults with non-specific chronic cough, we suggest against the empirical use of LTRAs (very low quality of evidence, conditional recommendation). Short-term ICS therapy is a preferred option over LTRAs as empirical treatment targeting asthmatic cough in non-specific chronic cough. However, LTRAs might be more suitable for patients with difficulty in using inhalers. As with the use of ICSs, objective documentation of asthmatic or eosinophilic cough justifies long-term treatment. Otherwise, only short-term (2-4 weeks) treatment is recommended.
What others are saying for adults
The 2004 ERS guidelines suggested LTRAs as potential add-on therapy for patients that achieve only a partial response to initial empirical corticosteroid therapy.15 The 2006 ACCP guidelines recommended LTRAs as an add-on therapy for patients with asthmatic cough that is refractory to ICSs and bronchodilators. The use of LTRAs as a monotherapy for asthmatic cough was uncertain.14
Summary of evidence for children
Our own systematic review identified one RCT of 63 patients aged 2 to 6 years with asthma-like symptoms (wheeze, cough, and/or shortness of breath),36 who were randomly allocated to receive fluticasone (100 μg twice daily; 25), montelukast (4 mg once daily; 18), or a placebo (20) for 3 months. The primary outcome was the daily symptom score (wheeze, cough, and shortness of breath) as recorded by caregivers in a symptom diary. Of the 11 children in the “cough only” subgroup, only 6 (5 in montelukast group and 1 in placebo group) had fulfilled the study criteria of non-specific chronic cough. There was no difference in clinical efficacy or adverse events between groups, but the effect of the intervention could not be estimated because the sample size was too small.
A single cohort study was found of 22 children (13 boys and 9 girls) aged 4 to 8 (median 5) years with non-specific cough for more than 3 weeks.37 In 14 children (68%), the cough ceased during the third week of treatment with montelukast (5 mg once daily). However, this result has to be interpreted with caution in the context of methodological problems such as biased subjective reporting, the placebo effect, and the period effect.
Recommendation for children
Currently, there is no reliable evidence to draw definite recommendations. When using LTRAs in children with non-specific chronic cough, careful considerations of cost and risk/benefits are needed until there is sufficient data to determine the efficacy of LTRAs in these children. Given the morbidity rate associated with non-specific chronic cough, evaluations are needed to assess the efficacy and safety of LTRAs for non-specific chronic cough in children.
Q4. Should PPIs be used to treat non-specific chronic cough? (in adults)
Summary of evidence
Two RCTs were identified.38 Our meta-analysis found no significant benefits from PPI treatment against subjective cough frequency or severity scores. Of note, although statistically insignificant, the study by Faruqi and colleagues38 found greater benefits of PPIs for a subgroup with dyspeptic symptoms as compared to of subgroup without.
In the literature, the effects of PPIs on cough were only demonstrated in patients with acid reflux, which is plausible considering the mechanisms of action. A meta-analysis by Kahrilas et al.39 indicated that PPIs may be effective only in patients with acid reflux. Meanwhile, there exists a global concern of PPI overuse. Use of PPIs without proper indications is prevalent in the community40 and may lead to potential risks of complications and high medical costs. Observational and large database studies suggest potential risks from PPI treatment, which include pneumonia, fracture, Clostridium difficile-associated diarrhea, hypomagnesia, dementia, and chronic renal diseases; however, the causal relationships were mostly unconfirmed.41
Recommendation
For adults with non-specific chronic cough, we suggest against the empirical use of PPIs (moderate quality of evidence, conditional recommendation).
What others are saying for Adults
The recommendation for the empiric use of PPIs has recently been revised in international guidelines. The 2016 ACCP guidelines recommended against the use of PPI therapy alone because of the unlikelihood to resolve suspected chronic cough in adult patients due to reflux-cough syndrome.42 It recommended the treatment include: 1) diet modification to promote weight loss in overweight or obese patients; 2) head of bed elevation and avoiding meals within 3 hours of bedtime; and 3) for patients who report heartburn and regurgitation, PPIs, H2-receptor antagonists, alginate, or antacid therapy sufficient to control these symptoms.42
II. DIAGNOSTIC TEST FOR CORTICOSTEROID-RESPONSIVE COUGH IN CHRONIC COUGH
Background
Asthma and eosinophilic bronchitis are 2 specific conditions that respond well to ICS treatment.43 These are common and important considerations in Korean patients with chronic cough, accounting for about half of adult cases according to a recent literature review.44 Unlike rhinitis- or reflux-associated cough, asthma and eosinophilic bronchitis can be objectively defined by methacholine challenge and induced sputum analysis.4546 However, these conventional tests are technically demanding and sometimes difficult for patients. Therefore, there is a high unmet need for easy and convenient alternative tests to predict steroid-responsive cough conditions.
Nitric oxide is a biological mediator generated from the airway epithelium and is up-regulated by interleukin (IL)-4 and IL-13.47 Likewise, FeNO levels have been shown to well reflect the degree of type 2 airway inflammation and to predict corticosteroid responsiveness in patients with respiratory symptoms.48 The greatest advantage of measuring FeNO levels is its simple, rapid, and non-invasive nature, potentially enabling the test to be widely applied in clinical practice.
Q5. Should FeNO measurement be used to predict asthma in chronic cough? (in both adults and children)
Summary of evidence for adults
A total of 10 studies were identified.49 Meta-analyses found a moderate accuracy of FeNO measurement to predict cough variant asthma with an area under the curve of 0.87 (95% confidence interval [CI], 0.83-0.89). Of note, specificity (0.85; 95% CI, 0.81-0.88) was higher and more consistent than sensitivity (0.72; 95% CI, 0.61-0.81). The optimal cutoff levels of the 10 included studies mostly ranged between 30 and 40 ppb. Because FeNO measurement is convenient and non-invasive,50 the guideline committee agreed that the test poses no safety concern.
Recommendation for adults
For adults with chronic cough, we suggest the use of FeNO measurement to predict asthma (moderate quality of evidence, conditional recommendation). FeNO measurement may be particularly useful when conventional diagnostic tests for asthma (such as methacholine challenge) are not available or patients have difficulty in performing the tests. However, it should be noted that the utility of FeNO is just to characterize the nature of airway inflammation (and thus can predict the anti-inflammatory treatment responses), but is not to confirm the diagnosis of asthma.51 Asthma is increasingly recognized as a heterogenous condition52 and is not definable by the presence of type 2 inflammation alone. Elevated FeNO levels in chronic cough patients with normal chest X-rays may suggest not only cough variant asthma but also eosinophilic bronchitis.53 In addition, unlike in patients diagnosed as asthma, there is no sufficient evidence to suggest optimal duration for anti-inflammatory treatment in chronic cough patients with high FeNO levels.
Summary of evidence for children
A total of four studies were identified.54555657 All were conducted in Chinese children. Our meta-analyses found a similar pattern in diagnostic accuracy between children and adults, with a sensitivity of 0.73 (95% CI, 0.46-0.90) and specificity of 0.96 (95% CI, 0.93-0.98). Again, high and consistent specificity was the strength of this test.
Recommendation for children
For children with chronic cough, we suggest the use of FeNO measurement to predict asthma (low quality of evidence, conditional recommendation). FeNO measurement may be particularly useful for younger patients who find it difficult to perform the bronchial challenge test. However, it should be noted that FeNO levels well reflect airway inflammation, but do not directly indicate a diagnosis of a specific disease.50
Q6. Should FeNO measurement test be used to predict eosinophilic bronchitis in non-asthmatic chronic cough? (in adults)
Summary of evidence
Only 4 studies of adult patients with non-asthmatic chronic cough (usually defined as negative methacholine challenge response) were identified.49 The estimated diagnostic accuracy for predicting sputum eosinophilia was moderate and specificity was higher than sensitivity, but neither were consistent (sensitivity: 0.72, 95% CI, 0.62-0.80; specificity: 0.83, 95% CI, 0.73-0.90). Similar findings were demonstrated in a meta-analysis of asthma patients.58 Possible observer variability in conducting and interpreting the data collected from induced sputum analyses might underlie such inconsistencies.
Induced sputum analysis is the gold standard test to diagnose eosinophilic bronchitis46 and is clinically useful to predict steroid-responsive cough.43 However, the utilization of this test has been mostly restricted to tertiary hospitals because of its technically demanding nature and requirement for specialized instruments and personnel.4650 Therefore, the guideline committee recognized that an alternative induced sputum test is practically necessary and decided to adapt the data from Korean populations to formulate a recommendation. A Korean study by Oh and colleagues53 found that 32 ppb as the optimal cutoff level to differentiate eosinophilic bronchitis.
III. EMPIRICAL ANTIBIOTICS FOR CHRONIC WET COUGH IN CHILDREN
Background
Protracted bacterial bronchitis (PBB), first described in 2006,59 is now recognized as an important cause of chronic wet cough in children. The original criteria of PBB were: 1) the presence of chronic wet cough; 2) response to antibiotics (amoxicillin-clavulanate) within 2 weeks of use; and 3) lower airway infection, as defined as the presence of respiratory pathogens at a density ≥ 104 CFUs/mL of bronchoalveolar lavage, in the absence of evidence of infection with Bordetella pertussis, Mycoplasma pneumoniae, or Chlamydia. Because it is not feasible for all children with chronic wet cough to undergo bronchoscopic examinations in routine clinical settings, criterion (3) has been replaced by absence of indicators suggestive of an alternative specific cause of cough. Although PBB also occurs in older children, patients with PBB are typically young (mean or median age 1.8-4.8 years).60 PBB has been incorporated into international pediatric cough guidelines.256162
Q7. Should empirical antibiotics be used to treat children with chronic wet or productive cough?
Summary of evidence
Our own systematic review identified one RCT of 50 children (mean age, 1.9 years; range, 6 months to <18 years) with chronic wet cough63 who were randomly assigned to receive either oral amoxicillin-clavulanate (45 mg/kg/day) or a placebo for 2 weeks. Cough resolution rates were significantly higher in children who received amoxicillin-clavulanate, as compared with those who received the placebo (48% vs. 16%, respectively, P = 0.015). Post-treatment, the median (interquartile range) verbal category descriptive score was significantly lower in the amoxicillin-clavulanate group as compared with the placebo group (0.5 [0.0-2.0] vs. 2.25 [1.15-2.9], respectively, P = 0.02). The bronchoalveolar lavage data from pre-treatment were consistent with PBB in a subgroup of children, with no significant difference between groups.
Recommendation
For children with chronic wet cough, we suggest the empirical administration of appropriate antibiotics for a period of 2 weeks, especially in children aged <6 years (low quality of evidence, conditional recommendation). Antibiotic selection should be based upon local sensitivity patterns. However, the proposed criteria for PBB are non-specific and may lead to substantial overdiagnosis. If chronic wet cough fails to respond to antibiotics, then further investigations are required to rule out other chronic suppurative lung diseases.
What others are saying
The 2008 BTS guidelines recommended a trial of physiotherapy and a prolonged course (e.g., 4-6 weeks) of appropriate antibiotics in children with PBB after exclusion of other underlying conditions.25 The 2017 ACCP guidelines recommended 2 weeks of antibiotics in children with chronic wet or productive cough without specific cough pointers and an additional 2 weeks of the appropriate antibiotics when the wet cough persists.64
IV. TREATMENT FOR UNEXPLAINED CHRONIC COUGH IN ADULTS
Background
A considerable proportion of adult patients with chronic cough (5%-40%) may not fit into any diagnostic categories or remain refractory to currently available treatment modalities, termed unexplained chronic cough (Table 1 and Fig. 2).65 There is increasing recognition that dysregulation of neural pathways leading to cough reflex hypersensitivity underlies this subgroup population.1066 Success from clinical trials with pain medications, such as opioids and gabapentin, also supports the notion that the neuropathic process is the key pathophysiological mechanism of unexplained cough.6768 Meanwhile, these populations may have some unique alterations in central nervous system processing of tussive stimuli and cough motor control. A recent series of functional brain magnetic resonance imaging studies demonstrated that these patients had increased signals in the descending modulatory system and reduced signals in brain areas related to cough suppression.69 In this regard, multi-dimensional behavioral therapy (or speech pathology therapy) may also have benefits in improving peripheral and central dysfunction in cough reflex pathways.
Q8. Should opioids be used to treat unexplained chronic cough?
Summary of evidence
Three studies were identified.677071 The best available evidence is found in the 4-week randomized placebo-controlled crossover study conducted by Morice and colleagues,67 which demonstrated that low-dose morphine (5 to 10 mg twice daily) significantly improved cough-related QOL and cough scores as compared to a placebo. Constipation, drowsiness, and nausea were the most common adverse events occurring in about half of patients treated with codeine or morphine. However, the long-term safety of opioid use for unexplained chronic cough remains unclear, thus further investigations are warranted. Due to genetic polymorphism in cytochrome P450 2D6 metabolism induced by long-term codeine use,72 the outcome of morphine, which is the end-product of codeine metabolism, is more predictable. However, only codeine is currently approved as an anti-tussive in Korea.
Recommendation
For adults with unexplained chronic cough, we suggest the use of low-dose opioids to control cough (low quality of evidence, conditional recommendation). Currently, codeine is the only approved opioid for anti-tussive use in Korea. Due to frequent side effects, careful consideration of the benefit-harm balance is recommended. The long-term benefits and harms warrant further investigations.
Q9. Should neuromodulators be used to treat unexplained chronic cough?
Summary of evidence
Two placebo-controlled trials and one head-to-head comparison (amitriptyline vs. codeine/guaifenesin) trial were identified.687374 In a randomized placebo-controlled parallel group trial of chronic refractory cough patients,68 Ryan and colleagues68 demonstrated that gabapentin had effectively improved cough-related QOL, cough severity visual analog score, and objective cough frequency. However, 31% of patients in the active group reported adverse effects, especially nausea and fatigue. In another randomized placebo-controlled parallel group study of chronic refractory cough, Vertigan and colleagues73 examined the efficacy of pregabalin as an add-on to speech pathology therapy and found that pregabalin significantly improved cough-related QOL and cough severity. However, there was no significant difference in cough frequency between the active and placebo groups. Adverse reactions, including blurred vision, cognitive change, dizziness, weight gain, and sleep disturbance, were also more frequent in the pregabalin-treat group.73 A study by Jeyakumar et al.
74 reported greater efficacy of amitriptyline, a tricyclic antidepressant, as compared to codeine/guaifenesin. However, the study was not placebo-controlled and also had limitations in allocation concealment and sample size.74
Recommendation
For adults with unexplained chronic cough, we suggest the use of gabapentin, pregabalin or amitriptyline (moderate quality of evidence, conditional recommendation). However, the use of these agents as antitussives has not been approved in Korea. As adverse reactions were very frequent, shared decision making with patients based on the benefits and harms is important. Long-term safety warrants further investigation.
What others are saying
The 2016 ACCP guidelines suggested a therapeutic trial of gabapentin for treatment of unexplained chronic cough, as long as the potential side effects and risk-benefit profiles are discussed with patients before use of the medication and there is a reassessment of the risk-benefit profile at 6 months before continuation.17
Q10. Should multi-dimensional behavioral therapy (or speech pathology therapy) be used to treat unexplained chronic cough?
Summary of evidence
Two RCTs were identified.7576 Vertigan and colleagues75 demonstrated that a 2-month regimen of speech pathology therapy significantly improved subjective cough scores as compared to a conventional health management regimen (relaxation, stress control, exercise, and diet). A study by Chamberlain Mitchell and colleagues76 also found that speech pathology therapy had effectively improved cough-specific QOL, cough frequency, and cough severity visual analog score. Of note, the benefits were sustained for more than 2 more months after the completion of therapy.76 No adverse effects were reported. Given the non-pharmacological nature of this therapy, the guideline committee agreed that there is likely no major safety concern.
Recommendation
For adults with unexplained chronic cough, we suggest the use of multi-dimensional behavioral therapy (or speech pathology therapy) (very low quality of evidence, conditional recommendation). At present, there is no standardized protocol for Korean patients.
What others are saying
The 2016 ACCP guidelines suggested a therapeutic trial of multimodality speech pathology therapy in patients with unexplained chronic cough.17
SUMMARY AND FURTHER RESEARCH NEEDS
The present guideline committee utilized systematic reviews and GRADE methodology to identify the best available evidence on the management for chronic cough in Korean patients. Through a comprehensive evidence synthesis process, we made recommendations for various diagnostic and therapeutic tools, including empirical treatments for non-specific and unexplained chronic cough, empirical antibiotics for chronic wet cough in children, and FeNO measurement to predict corticosteroid-responsive cough conditions (Table 3, Figs. 2 and 3).
However, the evidence was very sparse in most of our PICO questions, which is in marked contrast to the high burden of chronic cough in the community and clinics.14 In the absence of high-quality evidence, our guideline panel, nonetheless, formulated clinical guidelines, particularly for use in primary care. The United States Preventive Services Task Force stated77: “Decision makers do not have the luxury of waiting for certain evidence. Even though evidence is insufficient, the clinician must still provide advice, patients must make choices, and policy makers must establish policies.” In regard to the overall weak quality of evidence, most of our recommendations are inevitably conditional. Overall, the lack of evidence indicates a major unmet need for primary studies of patients with chronic cough. Considering the difference in epidemiology and clinical settings between regions, further definitive evidence should be generated from Korean populations. Our recommendations will be revised when new evidence becomes available.
 XML Download
XML Download