

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bronchial hyperresponsiveness (BHR) is one of the main features of asthma,1 but is also observed in some cases of rhinitis2 even in members of the general population with no symptoms. The prevalence of BHR has been reported variously from 10.6% to 78.2%, which was affected by subject age, population characteristics, provocation method and cutoff.345678910 BHR is associated with later asthma development in asymptomatic subjects,11 and its persistence is associated with allergic sensitization, a family history of allergic diseases and the asthma severity at diagnosis.121314 In Korea, BHR had been assessed with methacholine. The US Food and Drug Administration (FDA)-approved drug methacholine chloride (Provocholine®) began to be imported to Korea in 2015. Provocholine has now replaced all other methacholine agents in use in Korean hospitals.
Pulmonary function tests cannot be reliably performed until the age of 7, and BHR can also be precisely assessed in a traditional way from this age. The presence of BHR in children aged 6–7 years is known to be associated with the subsequent development of asthma.15 On the other hand, children with non-specific transient wheezing at the age of 7 years show a different clinical course from true asthmatics. Although some previous studies have evaluated the prevalence and risk factors for BHR in 7-year-old Korean children, they involved either small sample sizes or populations restricted to only 1 region, and therefore, cannot be regarded as nationally representative.34 Moreover, all previous data on this subject were derived from analyses of methacholine chemicals that are no longer in clinical use.
In our present study, we aimed to evaluate the prevalence of BHR to Provocholine and its risk factors in a large 7-year-old cohort from the general population adopted from the Panel Study on Korean Children (PSKC), a nationwide birth cohort study.16
MATERIALS AND METHODS
Study participants
We enrolled our current study participants from the PSKC birth cohort which we had previously established to provide nationwide longitudinal data on childhood development.16 This birth cohort recruited 2,078 mother-baby dyads using 2-step stratified random sampling across the whole nation in 2008 and has followed these subjects annually. A total of 1,577 children were followed in 2015. Of these subjects, 633 underwent laboratory screening for respiratory allergic diseases at the 16 participating regional hospitals in the cohort study. These tests included skin prick tests, blood tests, standard spirometry and a bronchial provocation test with Provocholine (Provocholine®; Methapharm Inc., Ontario, Canada). In addition, detailed histories were taken and physical examinations were conducted.
The Institutional Review Board of Asan Medical Center reviewed and approved the study protocol (IRB No. 2015-0907). Written consent was obtained from all parents and guardians following a detailed explanation of the study.
Recording of clinical data
The physicians at each regional study hospital that conducted the laboratory screening and recorded the information mostly comprised board-certified pediatric allergists. Detailed histories of the subjects were taken to verify the history of asthma, allergic rhinitis, atopic dermatitis, and other allergies and record the differential diagnosis in each case. Physical examinations were conducted to evaluate past and present allergic diseases. Current asthma was defined as a wheezy episode within the prior 12 months and a diagnosis of asthma by a physician.
Pulmonary function test, bronchial provocation test and measurement of serum total immunoglobulin E (IgE)
The study subjects underwent pulmonary function testing according to the 5-breath dosimeter protocol, which is the standard bronchial provocation test protocol suggested by the American Thoracic Society (ATS).10 All study centers used automated atomizer, with most centers using the DeVilbiss 646 nebulizer with a solenoid valve set to remain open for 0.6 seconds. The participants were requested to stop any medication that might influence the lung function results for at least 1 week prior to the test. The subjects were trained to conduct spirometry in a reproducible way (i.e., a coefficient of variation of the forced expiratory volume in 1 second [FEV1] did not exceed 5% in 3 consecutive flow-volume curves) before they were allowed to proceed to the bronchial provocation test.
The bronchial provocation test was conducted in accordance with internationally standardized guidelines.11 Briefly, fresh solutions of Provocholine were prepared in buffered saline solution at concentrations of 0.0625, 0.25, 1, 4 and 16 mg/mL. A dosimeter, triggered by a solenoid valve set to remain open for 0.6 seconds, was used to generate aerosol from a compressor with pressurized air at 20 pounds per square inch. Subjects inhaled normal saline until the lung reached its maximum volume capacity and held their breath for approximately 5 seconds, which was repeated 5 times. We measured the baseline FEV1 at 90 seconds from the fifth saline inhalation. Provocholine was then inhaled 5 times at each concentration, and the FEV1 was measured in the same manner until it showed a decrease of more than 20% compared to the baseline or the subjects reached the final Provocholine concentration of 16 mg/mL. The provocative concentration of Provocholine that caused a 20% decrease in the baseline FEV1 (PC20) was thereby calculated. In accordance with the internationally standardized guidelines for bronchial challenge test,17 those who had respiratory symptoms (within 4 weeks) or consumed medicine/food that may affect bronchial responsiveness were excluded from the test.
Blood was also withdrawn from each child at the hospital visit to measure the total serum IgE level by fluorescent enzyme immunoassay (ImmunoCap™; Phadia AB, Uppsala, Sweden).
Definition of current asthma and BHR to Provocholine
Current asthma was defined as both physician-diagnosed asthma-ever and a wheezy episode during the prior 12 months on the medical records. Risk factors for current asthma were analyzed using the responses to the 2015 questionnaires for the PSKC cohort. To compare its prevalence with those reported in prior studies, we defined BHR to Provocholine in our current series in a dual way i.e., we adopted the PC20 cutoff at both < 16 and < 8 mg/mL.8
Statistical analysis
Statistical analyses were conducted using SPSS version 23 (SPSS Inc., Chicago, IL, USA). The prevalence of current asthma and BHR to Provocholine are presented as mean values with a 95% confidence interval (CI). The χ2 test was conducted to compare subjects who visited a regional hospital and those who did not. The receiver operating characteristic (ROC) curve was applied to evaluate the best BHR cutoff for diagnosing current asthma. The χ2 test for trend was adopted to evaluate the trend of increasing prevalence of BHR and increasing serum total IgE. Logistic regression analyses were conducted to investigate risk factors affecting BHR and current asthma, and the odds ratio (OR) and 95% CI were calculated with adjustment for the following confounders: sex, maternal education levels, history of second-hand smoking, residential area and economic status.
RESULTS
Characteristics of the study participants
A flow chart for the subjects analyzed in this study is shown in Fig. 1. Among the 2,078 subjects recruited in the initial PSKC birth cohort, 1,577 including 809 boys and 768 girls attended the 2015 annual follow-up. To participate in the present study, 633 children visited the regional study hospitals where 559 subjects reliably completed the bronchial provocation test. Table 1 lists the characteristics of subjects who visited regional study hospitals compared to the PSKC subjects who declined to participate. The baseline characteristics were not significantly different between these 2 groups other than a previous history of bronchiolitis and the use of antibiotics in infancy.
Fig. 1
Flow chart of the study subjects.
PSKC, Panel Study on Korean Children; PFT, pulmonary function test.

Table 1
Characteristics of the whole PSKC cohort stratified by hospital visit for allergic testing

Lung function parameters and the prevalence of BHR and asthma in a general population of Korean 7-year-old children
Table 2 presents the lung function parameters and prevalence of BHR in subjects that completed the whole evaluation (n = 559), and the prevalence of asthma in the total population of children (n = 633) who attended the 16 regional hospitals for these laboratory evaluations. Although pulmonary function with spirometric parameters (forced vital capacity [FVC], FEV1 and FEV1/FVC) were significantly elevated in the boys compared with the girls, the prevalence of BHR did not differ by sex. A BHR to Provocholine, defined as a PC20 of < 16 mg/mL, was found in 25.8% (144/559) of these subjects, drawn from a general population of Korean children. When we adjusted the BHR cutoff to a PC20 of < 8 mg/mL, this prevalence decreased into 17.2% (96/559). There were no statistical differences between boys and girls in the prevalence of BHR. In the physician-verified records for these subjects, the prevalence of ever-diagnosed asthma, wheeze within the previous 12 months, and current asthma were 7.7% (48/625), 5.2% (32/620), and 3.2% (20/619), respectively.
Table 2
Lung function parameters, prevalence of BHR and asthma in the study subjects

BHR cutoff values for diagnosing current asthma
A ROC curve of the BHR to Provocholine for diagnosing current asthma in children is shown in Fig. 2. When we set BHR cutoffs at PC20 values of 16 and 8 mg/mL, the sensitivity remained unchanged at 47.1%, and the specificities were 74.9% and 83.8%, respectively. The optimal BHR cutoff value for diagnosing current asthma in children was a PC20 of 5.8 mg/mL with a sensitivity of 47.1%, specificity of 87.4%, positive predictive value of 10.7% and negative predictive value of 98.1%.
Fig. 2
ROC curve evaluation of the BHR cutoff used to diagnose current asthma in 7-year-old children.
ROC, receiver-operating-characteristic; BHR, bronchial hyperresponsiveness; AUC, area under the ROC curve; PC20, provocative concentration of Provocholine that caused a 20% decrease in the baseline FEV1; FEV1, forced expiratory volume in 1 second.
*Cutoff values for Provocholine PC20 provided the best combination of diagnostic sensitivity and specificity; †Provocative concentration causing 20% fall in FEV1.

Risk factors for BHR and current asthma
Table 3 lists the risk or associated factors for current asthma and BHR. The risk factors for BHR at a PC20 <16 mg/mL were atopic dermatitis diagnosis (adjusted OR [aOR], 1.61; 95% CI, 1.02–2.53) and current dog ownership (aOR, 2.33; 95% CI, 1.03–5.25). The risk factors for current asthma, however, were found to be quite different and included an allergic rhinitis diagnosis (aOR, 4.78; 95% CI, 1.30–17.58), history of bronchiolitis before the age of 3 (aOR, 3.95; 95% CI, 1.55–10.05), recent use of analgesics/antipyretics (aOR, 5.40; 95% CI, 1.21–24.14) and maternal history of asthma (aOR, 9.34; 95% CI, 1.98–44.10).
Table 3
Risk factors for current asthma or BHR in the study subjects (n = 559)

Data shown are aOR* (95% CI). Control group of current asthma: All subjects who are not defined as current asthma. Control group of PC20 < 16 mg/mL: All subjects who are not defined as PC20 < 16 mg/mL (which is the same as the group of PC20 ≥ 16 mg/mL). Control group of PC20 < 8 mg/mL: All subjects who are not defined as PC20 < 8 mg/mL (which is the same as the group of PC20 ≥ 8 mg/mL).
BHR, bronchial hyperresponsiveness; NA, not available; AR, allergic rhinitis; FA, food allergy; AD, atopic dermatitis; IgE, immunoglobulin E; CI, confidence intervals; aOR, adjusted odds ratio; PC20, provocative concentration of Provocholine that caused a 20% decrease in the baseline FEV1; FEV1, forced expiratory volume in 1 second.
*Adjusted by sex, maternal education levels, parental history of allergic diseases, history of second-hand smoking, residential area, and economic status; †Adjusted by sex, maternal education levels, history of second-hand smoking, residential area, and economic status, but excluding parental history of allergic diseases; ‡P < 0.05; §P < 0.01.
Correlation between BHR and IgE
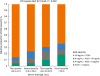
Fig. 3 shows the proportion of subjects with BHR stratified by IgE quartile. A trend towards a higher proportion of subjects with more severe BHR in the higher IgE quartiles was observed (χ2 test for trend <0.001).
DISCUSSION
We found, in our current analysis of 7-year-old Korean children from the general population, that the prevalence of current asthma, ever-diagnosed asthma by physicians and wheezy episode during the prior 12 months was 3.2%, 7.7%, and 5.2%, respectively. The prevalence of BHR assessed by exposure to Provocholine was 17.2% and 25.8% when we applied a PC20 cutoff of < 8 and < 16 mg/mL, respectively. The optimal Provocholine PC20 cutoff point for discerning current asthmatics was calculated as 5.8 mg/mL. The risk factors for BHR were determined to be a diagnosis of atopic dermatitis and current dog ownership, whereas those for current asthma included a diagnosis of allergy rhinitis, recent use of analgesics/antipyretics, a history of bronchiolitis at an age of < 3 years and a maternal history of asthma. Our study is the first to evaluate the prevalence, risk factors and appropriate cutoff value for the BHR to Provocholine in a general population of 7-year-old Korean children attending a birth cohort follow-up study.
When we calculate the prevalence of asthma, the way asthma is defined as well as the demographic profile of the affected subjects can have a large effect on this.181920 Since the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire is well-validated, it has been widely applied in most previous epidemiologic studies of allergic diseases. The difference in our current investigation, however, is that we, as a group of pediatric allergy specialists, verified the ISAAC questionnaire items to raise its diagnostic accuracy by directly taking a detailed history from our subjects. As a result, the prevalence of asthma, which we defined by a wheezing episode during the previous 12 months, was 5.2% in our current study cohort which is slightly lower than those reported in previous ISAAC questionnaire-based domestic studies in children aged 7 years. In a previous cross-sectional survey19 of 4,003 children aged 6–7 years from a random selection 45 primary schools across Korea, a 10.3% prevalence of asthma symptoms was reported. In that cross-sectional survey based on the ISAAC questionnaire, however, asthma symptoms were defined as any experience of wheezing in the lifetime of the child in addition to a wheezing episode within the previous 12 months. In a 2008 study20 of elementary school students from Seoul, the prevalence of wheezing within the previous year in 7-year-old children was 6.5% and thus similar to our current observation. Notably, however, that 2008 study population was limited to the Seoul region. Data obtained from elementary school students aged 7 to 12 years across Korea in 1995 and 200021 indicated an asthma prevalence of 3.2%–3.3% based on the history of asthma treatment within the previous 12 months. This finding is comparable to the 3.2% prevalence of current asthma in our current study which we defined as physician diagnosed asthma plus associated symptoms within the previous 12 months.
The prevalence of the BHR to Provocholine in our current study series was 25.8% and 17.2% when we adopted PC20 cutoff values of < 16 and < 8 mg/mL, respectively. There have been only 2 previous studies that included Korean children of the same age as our current subjects and these earlier investigations reported a prevalence of BHR to methacholine of 16.7% and 20.1%, respectively. One of these prior studies3 investigated the prevalence of BHR in 2,067 children from elementary and middle schools located in Seoul between 2011 and 2012, including 210 children aged 7 years. The BHR prevalence in that study using a methacholine PC20 of ≤ 8 mg/mL was reported as 16.7%. However, that analysis was also limited to the Seoul area and included a relatively small population of children compared to our current cohort. The other domestic Korean study3 analyzed the BHR prevalence in 7-year-old children based on the Children's Health and Environmental Research (CHEER) study, a nationwide cohort study that enrolled subjects from January 2005 to December 2006. In that particular report, 2,491 children (7.5 ± 0.9 years) were investigated, and the BHR prevalence to methacholine at a PC20 of < 8 mg/mL was approximately 20.1% which is comparable to the 17.2% found in our present analysis.
Among the relevant studies from outside Korea, the findings from an Australian birth cohort study6 are comparable to our current results. That birth cohort of 537 six-year-old children was enrolled from the antenatal clinic of a tertiary maternity hospital and reported a BHR prevalence of 78.2% at a cutoff of < 16 mg/mL, which is significantly higher than the 25.8% level in our current study at the same cutoff. Notably, however, the asthma prevalence is higher in western countries, and is in fact 2 times higher in Australia than in Korea. The younger age of the Australian participants and the fact that they were enrolled from an antenatal clinic may also underlie this discrepancy in the BHR prevalence.
The risk factors for current asthma and BHR were found not to be identical in our current analyses. Asthma is affected by genetic backgrounds and environmental factors, and the recent increase of allergic respiratory diseases due to environmental pollution is a serious social issue.22 Although only some studies to date have evaluated risk factors for BHR, structural factors including the baseline airway caliber, the age and sex of the subjects, and allergic factors including higher serum eosinophil counts and fractional exhaled nitric oxide (FeNO) are known to increase this risk.2324 Since families share both genetic traits and environmental factors, the familial history can also affect the presence and persistence of BHR. In our current study, allergic factors such as a diagnosis of atopic dermatitis and current dog ownership were found to elevate the risk for BHR, which paralleled the subgroup prevalence of BHR based on an elevated IgE. On the other hand, other factors less related to atopy such as the history of bronchiolitis at the age of < 3 years and the recent analgesic/antipyretic intake were found to be associated with the risk of current asthma. Multiple studies have identified sensitization of aeroallergen, respiratory infections, maternal asthma history and passive smoking252627 as the factors significantly associated with BHR, and these factors are similar to the known risk factors for asthma. However, a study on BHR in children showed that at 10 years of age, BHR has a narrower risk profile than asthma,24 suggesting that the risk factors for asthma and BHR may be distinct from each other. In our current analyses, history of bronchiolitis before 3 years of age and recent use of analgesics or antipyretics within 12 months were associated with current asthma, but not with BHR. Current dog ownership was not related to current asthma, but had relevance with BHR, suggesting that the effect of pet ownership on respiratory tract is complex. Although the reason for these differences is not yet clear due to the lack of appropriate biomarkers, we speculate that the different profiles of the subjects with BHR and symptomatic asthma may play a role.
Another interesting finding from our present analysis was the low sensitivity and specificity of BHR for diagnosing current asthma. Approximately half of the current asthmatics in our cohort did not present BHR to Provocholine. Although typical asthma symptoms such as cough, wheeze and chest tightness are known to originate from the excessive narrowing that typically constitutes BHR in older children, asthma-compatible symptoms can occur in the absence of excessive-to-baseline (i.e., more than 20%) airway narrowing in 7-year-old children who are still in the process of respiratory system growth and development.28 However, asymptomatic BHR is another issue which is currently defined as a temporarily elongated BHR associated with infection29 or as subclinical asthma,30 but the proportion of total-to-asymptomatic BHR cases is too high to be ignored. A different definition for confirming BHR should be considered and that is why we tried to adjust the BHR cutoff to obtain a more clinically relevant test. Our ROC curve analysis indicates an optimal BHR cutoff of PC20 < 5.8 mg/mL with a sensitivity of 47.1% and a specificity of 87.4%. It is notable that another Korean study reported a cutoff of 9.1 mg/mL in 7-year-olds.31 This discrepancy may involve different definitions of asthma, types of methacholine chloride used, and other potentially unadjusted variables. Further studies are warranted, therefore, to verify whether the current guidelines for a BHR assessment are adequate for diagnosing asthma32 in younger children. As for BHR cutoff value, sensitivity did not significantly change when the cutoff value was increased from 5.8 to 16 mg/mL (Fig. 2). There were no current asthmatics that had PC20 in the range from 5.8 to 16 mg/mL, which suggests that current asthmatics in this age group is a heterogenous set of conventional BHR-positive and BHR-negative asthmatics, which are a unique, age-specific subgroup with distinct pathophysiologic features.
There were several limitations in our present study. We defined current asthma using the epidemiological criteria, but we assume that pediatric allergy specialist's interview can compensate for some of the limitations of the ISSAC questionnaire. This method should be validated in future studies. Also, it was possible that the subset of PSKC birth cohort subjects who attended a regional hospital for laboratory testing might have had more pronounced medical conditions than the subjects who declined to participate. This may have led us to overestimate the prevalence of BHR or current asthma in the general Korean population. In addition, the data collected on risk factors were largely dependent on the recall of the children's parents and caregivers, which could not be verified by the treating physician. However, our study also had some notable strengths. Even though we confined our evaluations to Korean children aged 7 years, our results can be considered nationally representative, which is the principal strength of our study design. Our enrolled subjects were participants in a birth cohort designed for the 7-year-old general population distributed across Korea. Moreover, we gathered BHR data on 559 of these subjects, which is a substantial sample size. In addition, every regional study hospital who contributed to these analyses followed the same protocols that meet the ATS criteria17 in the laboratory and used the same devices that are used in our own practice, which greatly contributes to the interpretation of the findings and wider applicability. Finally, our current study is the first to report on the BHR to the newly-introduced and now widely adopted methacholine chloride drug in Korea.
In conclusion, we observed that most 7-year-old children can reliably undergo the Provocholine challenge test. The prevalence of BHR (PC20 < 8 mg/mL) is 17.2% and, the cutoff value of PC20 to Provocholine is 5.8 mg/mL for the diagnosis of current asthma in 7-year-olds. Hence, the bronchial provocation test will be a useful clinical tool in our own practice in the future. It will still be necessary to evaluate the natural course of asthma and BHR to Provocholine through a long-term follow-up study.
 XML Download
XML Download