

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tuberculosis (TB) remains a major public health problem, causing significant morbidity and mortality worldwide.1 First-line antituberculosis drugs (ATD) with rifampin (RFP), isoniazid (INH), pyrazinamide (PZA), and ethambutol (EMB) are effective, but this regimen often causes serious adverse drug reactions, which result in discontinuing the scheduled treatment.2 Rashes induced by first-line ATD are common and major adverse reactions.3 ATD-induced maculopapular eruption (MPE) is the most frequent type of ATD-induced rash.4 The pathogenic mechanisms underlying ATD-induced MPE remain elusive, but predisposing genotypes may underlie susceptibility to ATD-induced MPE.5,6 We have explored the genetic risk factors to the development of ATD-induced MPE. In previous reports, we focused on metabolic enzymes and identified genetic variants in cytochrome P450 (CYP) 2C19 and CYP2C9 that contribute to ATD-induced MPE.4,6
The multidrug resistance 1 (MDR/P-glycoprotein/ABCB1) and multidrug resistance associated protein 2 (MRP2/ABCC2) genes Koreawere selected for this genetic association study as candidate risk markers of ATD-induced MPE based on their associated role and the findings of previous studies.7-10 The ATP-binding cassette (ABC) transporters are increasingly recognized as key determinants in adverse drug reactions and drug resistance.8 MDR1 is expressed in intestinal cells, the biliary canalicular membrane of hepatocytes, and the kidney.7 Furthermore, RFP is the classical inducer of MDR1, which decreases the clearance of co-administered drugs.11 MRP2, expressed on the bile canalicular membrane, hepatocyte7 and keratinocytes,12 plays an important role in the biliary excretion of various kinds of reactive metabolites and may regulate the efflux of substrates in the skin. ABC transporter C2 gene (ABCC2) polymorphisms that are functionally relevant and may impair the clearance of xenobiotics and their toxic metabolites have been identified.9,13,14 Therefore, it can be hypothesized that ABC drug transporters play an important role in ATD-induced MPE. To our knowledge, there is no published report of the associations between genetic polymorphisms of ABCB1 and ABCC2 and ATD-induced MPE. This study aimed to evaluate the genetic associations of ABCB1 and ABCC2 polymorphisms and haplotypes with the ATD-induced MPE in Korean patients with tuberculosis.
MATERIALS AND METHODS
Subjects
The genomic DNA used for the genotypes and the demographic data of 62 ATD-induced MPE cases and 159 ATD-tolerant controls were pooled from a previous study.6 Demographic data were described previously. Briefly, no significant differences in demographic parameters, such as age, sex, height and weight, or body mass index were found between case and control subjects. All patients with pulmonary TB and/or TB pleurisy were treated daily with a combination regimen including INH (300-400 mg daily), RFP (450-600 mg daily), EMB (600-800 mg daily), and PZA (1,000-1,500 mg daily) for two months and then without PZA for four or more following months, according to the treatment guidelines of the American Thoracic Society, Centers for Disease Control and Prevention, and the Infectious Diseases Society of America.15 Doses of each drug were adjusted based on the body weight of the patient. Patients with skin diseases before treatment, chronic renal failure, and chronic liver diseases, including alcoholic hepatitis, fatty liver disease, liver cirrhosis, and carriers of the hepatitis B or C virus, and non-adherence to the treatment, were excluded. All subjects provided informed consent and the study was approved by the Institutional Review Boards of each participating hospital. Patients were seen at regular intervals and questioned regarding symptoms related to adverse reactions to ATDs. In addition, an unscheduled visit occurred if a new symptom appeared. ATD-induced MPE was defined as the development of MPE after receiving first-line ATD and the disappearance of MPE after discontinuing ATD.
Selection of SNPs and genotyping
We selected the ABCB1 and ABCC2 single nucleotide polymorphisms (SNPs) for evaluation in this case-controlled analysis, as described previously.16 Briefly, we identified 10 SNPs with frequencies >2.0%. Of these, nine were selected as tagging SNPs for genotyping and further analysis. The selected SNPs were scored with the high-throughput single base-pair extension method (SNP-IT™ assay), using an SNPstream25K system customized to automatically genotype DNA samples in 384-well plates and provide a colorimetric readout (Orchid Biosciences, Princeton, NJ, USA). The ABCB1 and ABCC2 haplotypes and their frequencies were estimated using Haploview version 3.32 (http://www.broad.mit.edu/mpg/haploview/) in the analysis of the LD between SNPs in each gene.
Statistical analysis
Genotype frequencies were compared between patients with ATD-induced MPE and ATD-tolerant controls using a multivariate logistic regression analysis controlling for age and sex as covariates. We used three different analysis models (dominant model, recessive model, and allele model) to compare genotype frequencies. Hardy-Weinberg equilibrium was tested for using chi-square tests. All statistical analyses were performed using SAS (version 8.1; SAS Institute, Cary, NC, USA), and P values <0.05 were regarded as statistically significant.
RESULTS
Polymorphisms and haplotypes of ABCB1 in patients with ATD-induced MPE and controls
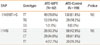
Of the two selected ABCB1 SNPs (-114918T>G and I1145I), none were significantly associated with the development of ATD-induced MPE (Table 1). In the ABCB1 haplotype analysis, no significant associations between the haplotypes of each gene and ATD-induced MPE were observed (data not shown).
Polymorphisms of ABCC2 in patients with ATD-induced MPE and controls
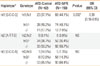
Among seven SNPs in ABCC2, IVS3-49C>T and I1324I were significantly associated with ATD-induced MPE (P=0.029 for the recessive model, OR=3.15, 95% CI: 1.09-9.11 and P=0.036 for the allele model, OR=0.029, 95% CI: 1.12-9.53, respectively). The genotype frequencies of the other five ABCC2 SNPs (-1774del>G, -1549G>A, -24C>T, V417I, and S978S) did not differ between cases and control subjects (Table 2).
Haplotypes of ABCC2 in patients with ATD-induced MPE and controls
Of three ABCC2 haplotypes (-1549G>A_-24C>T_IVS3-49C>T_V417I) with frequencies higher than 0.05, ht1[G-C-C-G] was significantly associated with ATD-induced MPE (P=0.032 for the dominant model, OR=0.39, 95% CI: 0.16-0.95; Table 3). Ht1[G-C-C-G] was present in 82.3% of the ATD-induced MPE group and 92.3% of the ATD-tolerant controls.
DISCUSSION
This is the first study to demonstrate an association between polymorphisms and a haplotype [G-C-C-G] of ABCC2 and ATD-induced MPE in Korean patients with tuberculosis. ABC transporters are transmembrane proteins that utilize the energy of ATP to transport several biological compounds across the membrane.13 ABCC2 is involved in the susceptibility of the drug response and toxicity. Genetic polymorphisms of ABCC2 are reported to alter the bioavailability of many drugs, such as cefazolin, erythromycin, levofloxacin, digoxin, fexofenadine, and nelfinavir.7 In addition, genetic variation of ABCC2 showed a strong association with the adverse drug reaction, including toxic liver injury,14 diclofenac-induced hepatotoxicity9 and a carbamazepine-induced neurological adverse reaction.10 Drug-induced MPE appears to be mediated by a delayed drug-hypersensitivity reaction, in which drug-specific T cells are activated in a major histocompatibility complex-dependent manner. After proliferation of a drug-specific T cell clone, T cells infiltrated the skin via unique homing receptors and showed cytotoxic activities.17 ATDs alone are incapable of activating the immune system. Instead, the drug or its metabolite must bind an endogenous protein before becoming immunogenic. Therefore, it can be speculated that drug transporters, which play important roles in the distribution and elimination of the drug or its reactive metabolites, are candidate genes for ATD-induced MPE.
Recent studies demonstrated that these genetic polymorphisms, such as HLA,18 GST,19 CYP2C9,5 and CD40 and CD40L,20 may be associated with susceptibility to drug-induced cutaneous reactions. In addition, we demonstrated that CYP2C19 and CYP2C9 genetic polymorphisms are significantly associated with the risk of developing ATD-induced MPE, not NAT2, CYP2E1, GSTM1 and GSTP1.4,6 The frequency of wild-type IVS3-49C>T and I1324I polymorphisms were much lower in patients with ATD-induced MPE compared to ATD-tolerant controls. These findings suggest a protective role for IVS3-49C>T and I1324I ABCC2 polymorphisms in the development of ATD-induced MPE. However, further functional studies are needed to clarify the precise role of these polymorphisms in the development to ATD-induced MPE.
Unlike this study, a previous report of ours found no association between ABCC2 polymorphisms and ATD-induced hepatitis.16 The inconsistency in the association between ABCC2 polymorphisms and the phenotypes of ATD-induced adverse reactions suggests that these associations are phenotype-specific. An increasing body of evidence confirms that associations between genotypes and drug-induced hypersensitivity reactions are phenotype-specific.6,21-24
A few limitations of this study should be addressed. First, our case-control results did not satisfy the criteria for Bonferroni significance. When applying the conservative Bonferroni corrections for multiple comparisons, the P values of IVS3-49C>T, I1324I and ht1[G-C-C-G] were smaller than the Bonferroni significance (0.007; a/number of comparison=0.05/7, 0.016; a/number of comparison=0.05/3). In our study, because we simply accepted P<0.05 for single haplotype comparisons, the risk of false positives (type I error) was increased. Second, owing to the small number of ATD-induced MPE cases, our analyses provided limited power and the conclusions should be interpreted with caution. However, we believe that our results have greater significance than previous reports. In our previous study, a haplotype of CYP2C9-CYP2C19 [T-A-T-C] was significantly associated with the development of ATD-induced MPE in the same groups.6 Third, we enrolled patients with ATD-induced MPE without identification of the culprit drug. Therefore, this may have masked the existence of significant associations between one specific ATD and ABCB1 and other ABCC2 polymorphisms. Finally, a growing list of drug transporters has been recognized, and the main drug transporters of specific ATDs remain unclear. Therefore, future studies are required to evaluate the possible associations between polymorphisms of other drug transporters and ATD-induced MPE.
In conclusion, we report here that IVS3-49C>T and I1324I polymorphisms and an ABCC2 haplotype [G-C-C-G] might be associated with susceptibility to ATD-induced MPE. These findings may facilitate development of models and tools using other risk markers for the prediction of ATD-induced MPE before prescribing anti-TB medications.

 XML Download
XML Download