

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Rhinitis is a chronic inflammatory disease of the upper respiratory airways characterized by the cardinal symptoms of nasal congestion, rhinorrhea, sneezing, and nasal itching.123 The prevalence of rhinitis in Korean elementary school students increased from 15.5% in 1995 to 28.5% in 2006.45 According to data gathered via a questionnaire from the International Study of Asthma and Allergies in Childhood (ISSAC), in 2010 the prevalences of rhinitis were 28.5%, 38.0%, 38.5%, and 35.9% in children 0 to 3 years of age, 4 to 6, 7 to 9, and 10 to 13, respectively.6 Allergic rhinitis (AR) is classified as a type of rhinitis and defined as rhinitis symptoms plus positive allergen sensitization.2 The prevalence of AR is combined with measures of overall rhinitis' prevalence, and it is difficult to differentiate AR from other types of rhinitis in most data sets.7
Rhinitis has a harmful influence on the physical, social, and psychological health of children and adolescents.389 Comorbidities of rhinitis are common and also have a significant influence on quality of life and health.3 These comorbidities, which affect both children and adolescents, include asthma, conjunctivitis, otitis media, rhinosinusitis, and pollen-food syndrome, and can be used as markers of possible rhinitis.37 Sleep disturbance is a comorbidity that often results in impaired school performance and has negative effects on the quality of life of adolescents.310 Moreover, some of the principal allergic diseases in children often coexist with rhinitis.611
Therefore, the impacts and costs associated with comorbidities of rhinitis should be considered in the management of rhinitis in the pediatric population. However, there are few studies on the comorbidities of rhinitis in children. In addition, little is known about the phenotypes, characteristics, and epidemiology of rhinitis, including AR, in Korean children and adolescents.
We sought to analyze the comorbidities and phenotypes of rhinitis in Korean children and adolescents and to investigate sensitized allergens and their variety according to age through a cross-sectional, multicenter study design based on a physician-targeted questionnaire.
MATERIALS AND METHODS
Study design and population
This is an epidemiological, cross-sectional, multicenter study intended to evaluate the comorbidities and phenotypes of rhinitis in children and adolescents. Data were collected retrospectively from patients aged less than 18 years who were diagnosed with rhinitis between January 2013 and January 2015 by pediatric allergy specialists from 11 hospitals in South Korea. We analyzed symptoms, classification according to the Allergic Rhinitis and its Impact on Asthma (ARIA) guideline, comorbidities, and allergen sensitization. This study was approved by the Institutional Review Board of all participating hospitals.
Study outcomes
NAR and AR
If the patients had more than one of the symptoms of rhinitis, such as sneezing, rhinorrhea, nasal obstruction, and nasal itching, they were diagnosed with rhinitis.2 AR was diagnosed by doctors if the patient tested positive for sensitization to inhaled allergens.2 Rhinitis without sensitization to any of the allergens tested was defined as NAR.2 Using the ARIA guideline, AR was classified into intermittent/persistent and mild/moderate-severe types. Duration of AR was classified as intermittent (sympsymptoms <4 days a week or for <4 consecutive weeks) or persistent (symptoms lasting more than 4 days a week and for more than 4 consecutive weeks).2 Severity of AR was classified as mild or moderate/severe depending on sleep disturbance; impairment of daily activities, leisure, sport, school, and/or work; and troublesome symptoms.2
Definition of comorbidities
Rhinitis in children and adolescents can frequently present with associated comorbidities, such as conjunctivitis, asthma, sinusitis, sleep disturbance, atopic dermatitis, otitis media, and oral allergy syndrome. Conjunctivitis was defined by symptoms (i.e., red, itchy, watery eyes and eye rubbing) and signs.3 Asthma was defined by symptoms (cough, wheeze, and exercise-induced bronchospasm) and spirometry results for those >6 years of age.3 Atopic dermatitis was diagnosed by doctors according to the criteria proposed by Hanifin and Rajka13 and the Korean diagnostic criteria.12 Otitis media was diagnosed after ear examination by physicians.14 Rhinosinusitis was defined as prolonged symptoms of nasal obstruction, purulent rhinorrhea or postnasal drainage, and complaints, such as headache, facial pain, or cough.3 Sleep problems comprised a history of disturbed sleep, snoring, apnea, tiredness, and irritability.3 Oral allergy syndrome (OAS, pollen–food syndrome) was defined as oral pruritus or swelling that occurred due to cross-reactivity between aeroallergens, such as birch pollen, and fruits and vegetables, such as apples.15
Allergic sensitization
Allergic sensitization was defined as a positive skin prick test (SPT) and/or positive specific IgE test for house dust mites (HDMs), animal dander (mostly cat and dog), and pollens by a multiple antigen simultaneous test (MAST) or an Immuno-CAP. In SPT, common environmental allergens as well as positive and negative controls (histamine and saline, respectively) are introduced into the skin by a needle, and any immediate reaction (wheal and erythema) were read after 15 to 20 minutes.216 Result of the SPT is considered positive when the wheal size of allergen (A) is larger than that of histamine (H) (A/H ratio ≥1), the grade higher than 3+, and ≥3 mm in average of the longest and the shortest diameters.161718 A specific IgE level of 0.35 kUA/L or greater on the Immuno-CAP system19 or more than class 3 by MAST was defined as a positive result.20
Statistical analysis
We investigated the relationship among symptoms, comorbidities, allergen sensitization, and severity and/or duration of NAR and AR in children and adolescents. All data are presented as number (n) and frequencies (%) for categorical variables, and mean and standard deviation (SD) for quantitative variables. Non-test patients were excluded when we compared the NAR and AR groups.
Pearson's χ2 test was used to evaluate 2×2 cross-table analyses. For 2×N cross-table analyses, the linear to linear χ2 test was used. All statistical analyses were performed using IBM SPSS ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
Demographic characteristics of subjects
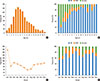
Eleven hospitals participated and 939 patients were recruited. Seven hospitals located in Seoul enrolled 645 patients, 3 hospitals located in Gyeonggi-do enrolled 203 patients, and 1 hospital located in Deagu enrolled 91 patients. All participating hospitals were located in an urban area. The patients consisted of 14.5% with NAR, and 68.3% with AR. The majority of the patients were boys (61.4% overall, 55.1% NAR and 63.2% AR). The mean age at presentation was higher in the AR than in the NAR group (7.5±3.4 vs 5.5±2.9 P<0.001; see Table 1). The peak age was 5 years old (126 patients, 13.4%) (Fig. 1A). A history of allergic disease in the family was reported for 681 patients (72.9%) and significantly more patients with a familial history had NAR (P=0.014) (Table 1). Twelve patients (1.3%) presented in infancy, and 514 (54.7%) patients were less than 6 years old (Fig. 1A). There were more AR patients even among those less than 1 year old (Fig. 1B). Most patients presented during the winter (December 9.2%, January 18.7% vs July 4.2%, August 4.8%) (Fig. 1C), and the distribution of AR and NAR did not vary by season (Fig. 1D).
Clinical characteristics of rhinitis
Nasal obstruction was the most common symptom in both NAR and AR, but significantly more patients with NAR (93.4%) than AR (86.7%) were affected (P=0.031) (Table 1). The number of patients who complained of sneezing was significantly larger in the AR (63.5%) than in the NAR group (52.2%) (P= 0.014) (Table 1). The frequency of rhinorrhea and nasal itching was not different between the NAR and AR groups. Multiple symptoms were present in most rhinitis patients. Two hundred and five (32.2%) AR patients and 48 (36.4%) NAR patients complained of all symptoms, including rhinorrhea, sneezing, nasal obstruction, and nasal itching (Fig. 2A and B).
Classification of AR
According to the ARIA classification, the most frequent type of AR was moderate-severe persistent AR (41.2%), followed by mild persistent (27.9%), moderate-severe intermittent (18.9%), and mild intermittent (12.1%) (Table 1). Sneezing and itching were more common in persistent rhinitis than in intermittent rhinitis (P<0.001 and P=0.001, respectively) (Table 2). Nasal obstruction was more common in both moderate-severe cases (P=0.001) and persistent cases (P<0.005) (Table 2). Patients with persistent AR had significantly more symptoms than those with intermittent AR (P<0.001) (Table 2).
Comorbidities of rhinitis
The most frequent comorbidity for patients with AR was rhinosinusitis (42.8%), followed by conjunctivitis (37.5%), sleep disturbance (33.4%), asthma (29.9%), atopic dermatitis (29.1%), otitis media (10.1%), and oral allergy syndrome (4.8%) (Table 1). In patients with NAR, sinusitis (38.2%) was also the most frequent comorbidity, followed by sleep disturbance (27.2%), conjunctivitis (11.2%), atopic dermatitis (35.1%), asthma (10.3%), and otitis media (3.8%) (Table 1). Conjunctivitis, asthma, and otitis media were significantly more common in the AR group than in the NAR group, but there was no difference between the groups in the other comorbidities (Table 1). In patients with AR, sleep disturbances were more common in moderate-severe rhinitis than in intermittent rhinitis (P<0.001). There was no significant relationship between severity and duration of AR and any other comorbidities, such as conjunctivitis, asthma, atopic dermatitis, otitis media, and sinusitis (Table 2).
Allergen sensitization in AR
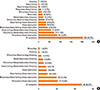
The proportions of children and adolescents sensitized to HDMs, pollen, animal dander, and allergens increased significantly from less than 5 years old to more than 12 years old (Fig. 3, 4A and B). However, it was noteworthy that the proportion of patients sensitized to HDMs peaked in 6 to 11 year olds. Furthermore, in the AR group, the proportion sensitive to HDMs decreased in the older children (P=0.027) (Fig. 4B).
DISCUSSION
There have been few large-scale investigations of clinical manifestations, including comorbidities and phenotypes, of rhinitis in Korean children and adolescents. Moreover, research including Korean adolescents is rare. As far as we know, this is the first multicenter study that showed a difference in comorbidities between NAR and AR in Korean children and adolescents. Patients with AR had more conjunctivitis (37.5%), asthma (29.9%), and otitis media (10.1%). Sleep disturbance was a critical comorbidity related to the persistence of AR in Korean children and adolescents. Moderate-severe persistent AR was the most common type of AR (using the ARIA classification) in our patients, and nasal obstruction was the most common symptom of AR in Korean children. We also found a significant association between age and inhalant allergens, which suggests the necessity of early diagnosis and intervention.
It is difficult to distinguish between AR and NAR through use of the ISAAC questionnaire because its diagnosis is not supported by specific IgE tests. In our study, AR and NAR were clearly defined by specific IgE tests. AR was more common, affecting 641 (68.3%) patients as compared to 135 (14.5%) patients with NAR, a trend that existed across most of the age groups. A Norwegian study reported a 72.8% prevalence of AR and 27.2% of NAR in 10 year-olds.7 A Korean study reported 76.9% AR vs 23.1% NAR.21 The prevalence reported in our study may be different those in from other studies due to not having inhalant allergen test data from all patients, particularly ≤5 years old. However, all adolescents more than 14 years old were examined with allergy tests, and 100% were positive in the 14 to 17 years old group. Considering that AR increased and NAR underwent remission with advancing years,22 our results are similar to other studies.
Until now, there has been little research into the comorbidities of AR in children in Korea. A recent investigation of comorbidities of AR from the Korea National Health and Nutrition Extermination Survey (KNHANES) reported the prevalence, risk factors, and comorbidities of rhinitis in an adult population.23 They reported asthma, chronic rhinosinusitis, and olfactory dysfunction were more prevalent in the AR group, and asthma was correlated to severity and atopic dermatitis. According to a study of a birth cohort of 2,024 children from Sweden, AR and NAR were associated with asthma, eczema, and food hypersensitivity, and 25% of 8-year-olds with AR also had oral allergy syndrome.22 A cross-sectional population survey in Korea found the percentage of patients with AR and asthma, and those with AR and atopic dermatitis were 4.7% and 8.7%, respectively, among 31,201 children between 0 and 13 years of age.6 Atopic dermatitis, asthma, and oral allergy syndrome were found in 29.7%, 24.1%, and 4.6%, respectively, of our patients. These high rates of comorbidities are probably due to the study's hospital-based design. A position paper from the European Academy and Allergy Clinical Immunology Taskforce on Rhinitis in Children recognized comorbidities of rhinitis, including conjunctivitis, asthma, impaired hearing, rhinosinusitis, sleep problems, and pollen-food syndrome.3
In our study, most rhinitis patients had one or more comorbidities, and patients with AR had significantly more comorbidities than patients with NAR. One study reported 11.8% of children with rhinitis had conjunctivitis, asthma, or atopic dermatitis.7 Although there was no significant association between conjunctivitis and age or severity of AR in our study, conjunctivitis was the most common comorbidity, affecting more than half of the children with AR in several European studies.724
Bronchial eosinophilic inflammation could be associated with an increase in nasal eosinophilic chemotactic factors and bronchial hyper-responsiveness (BHR), which are significantly related to AR.725 Our findings support the concept that AR and asthma are one airway disease.26 If allergen exposure in the nasopharynx is associated with secretion of histamine and allergic mediators, the Eustachian tube could be obstructed and sequentially cause middle ear effusion.2728 Allergic inflammation also contributes to the hypertrophy of lymphoid tissues, such as the adenoids and tonsils,27 explaining how AR could contribute to the development of otitis media and rhinosinusitis.7
The higher prevalence of moderate-severe persistent patients in our study may be the result of selection bias, as patients were recruited from secondary or tertiary hospitals. Unlike our results, intermittent AR was more prevalent in a population-based study in Spain.24
In our study, the most common AR symptom was nasal obstruction (86.7%), and the presence of nasal obstruction was significantly associated with both the severity and persistence of AR (Table 2). The importance of nasal obstruction is also noted in the Pediatric Allergies in an American survey as the main symptom in children.29 The authors collected information in on symptom burden, quality of life, productivity, disease management, and medication, and concluded that its burden on children in the United States has been significantly underestimated.29 Because nasal congestion is associated with sleep-disordered breathing and seems to be a major cause of sleep impairment in patients with AR, treatment to reduce nasal congestion has a positive influence on sleep.30
Like other chronic diseases, AR affects the quality of life in children by causing bothersome symptoms and comorbidities and by requiring medication use. There have been some trials to assess the quality of life in Korean children with AR by questionnaires.3132 Contents of the questionnaire involved the degree of discomfort caused by main symptoms, daily activity or sleep disturbance, and psychosocial problems. A substantial proportion of subjects (38.6%) complained of sleep disturbances, which can be caused by nasal obstruction.30 Sleep disturbance was the only comorbidity that was significantly associated with the persistence of AR (P<0.001) and marginally significantly associated with severity (P=0.056) in our study. The other comorbidities were not significantly related to AR classifications according to the ARIA guideline (Table 2).
The nose is anatomically and physiologically linked to the paranasal sinuses, pharynx, middle ear, larynx, and lower airway. Therefore, presentation of AR may be associated with mouth breathing and snoring with sleep problems, and chronic cough.33 First-generation H1 antihistamines can also cause sleep problems and performance impairment.33343536 In our study, a sleep disturbance questionnaire was filled out by patients and/or their parents, but objective tests, such as polysomnography, should be performed for accurate evaluation of sleep disturbance.
We identified an age-dependent increase in sensitization to inhalant allergens, but there was no significant correlation between the severity of AR and allergen sensitization. An Italian multicenter study comprising 1,360 children with AR showed that 84.9% were sensitized to more than 3 allergens and that there was a strong association between pollen induced AR duration and severity.17 Young children, including those less than 1 year of age, already had allergic rhinitis due to sensitization to HDMs (7 children, 58.3%) and pollen (3 children, 25%). HDM sensitization occurred from less than 1 year of age and increased until 6-11 years of age. The rate of HDM sensitization was 73.1% in all rhinitis patients, and 89.1% in AR patients. Sensitization rates to pollen or animal dander increased significantly with advancing age. The prevalence and changing patterns of allergen sensitization in our study are similar to those in other Korean studies.21 Although sensitization to pollen is reported to be related to AR, we did not confirm this finding in our study.3738
Atopic sensitization may be influenced by several environmental exposures occurring after infancy.39 The National Health and Nutrition Examination Survey (NHANES) in the USA announced that atopic sensitization to dust mites, plant-related allergens, or pets (dog or cat) affected 20.3%, 27.1%, and 15.7% of children, respectively.40 This implies that there is a big difference in the allergen sensitization rate and pattern in children between Korea and the USA, not surprising if the environment is supposed to be an important factor. On the basis of our study, both HDMs and pollen allergens should be evaluated in all Korean children even if less than 1 year old when doctors suspect the child has allergic sensitization.
Our study might be influenced by some limitations. First, 10 of the 11 hospitals are located in Seoul metropolitan area including Gyeonggi-do, and the geographic distribution of patients was biased toward Seoul. Therefore the study population is not truly representative of the Korean general population.
Secondly, there might be some heterogeneity across the methods of skin prick tests or serologic tests for specific IgE due to its multicentricity, and some patients were not evaluated by allergy tests, so that we could not confirm AR or NAR. Thirdly, a cross-sectional study design cannot clarify the role of risk factors in the natural course of a disease. However, our study investigated comorbidities of rhinitis and allergic sensitization from less than 1 year to 18 years old, and was a multicenter study. Therefore, it can be used as representative data in allergic rhinitis in children and adolescents in Korea.
In conclusion, this study revealed that AR was more prevalent than NAR and that moderate-severe persistent AR was the most frequent type in Korean pediatric populations. Nasal obstruction was an important symptom associated with the severity and persistence of AR. Sinusitis was the most common comorbidity, and sleep disturbance was associated with the severity of rhinitis. These findings may be helpful in developing a plan for the prevention and treatment of rhinitis and in improving the quality of life of Korean children and adolescents suffering from AR. Further nationwide and longitudinal studies will help understand the relationship between these diseases.




 XML Download
XML Download