

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bladder cancer is among the most common newly diagnosed cancer in the Western population, with an estimated 77,000 new cases diagnosed in the US in 2016 [1]. Following progression to muscle-invasive bladder cancer (pT2), curative treatment of choice is radical cystectomy including regional lymph node dissection [2]. From time of diagnosis Australian bladder cancer patients have a 5-year survival rate of approximately 58% [345]. Accordingly, there is an inherent need for improved treatment regimens for these patients. Organ-confined muscle-invasive bladder tumours are often complex with up to 25% having lymph node metastasis [6]. There is mounting evidence suggesting the addition of pelvic lymph node dissection (PLND) to radical cystectomy provides superior oncological outcomes compared to non-PLND cohorts. Specifically, lymphadenectomy provides improved cancer staging, prolongs time to disease recurrence and cancer-specific survival [78910111213]. As such, contemporary European Urological Association guidelines support radical cystectomy and regional lymph node dissection for curative treatment of muscle invasive bladder cancer [2].
The improved oncological outcomes following PLND have prompted changes to dissection practices, with clinicians adopting more extensive dissection templates [14]. The precise oncological benefits of varying dissection templates are unclear and this is reflected by uncertain guidelines. Current data suggests that more extensive dissection results in improved oncological outcomes [15]. However there may be no added oncological benefit to superextended dissection above the mid-upper third of the common iliac vessels [10]. There is still no consensus regarding the boundaries or nomenclature of a standard set of PLND templates [15]. We aim to investigate the impact of lymph node yield and dissection extent on oncological outcomes in an Australian cohort treated surgically for primary bladder cancer.
MATERIALS AND METHODS
1. Patients
Following Austin Health Human Research Ethics Committee approval, we conducted a 10-year multiinstitution, multisurgeon retrospective review (approval number: LR227-15). Informed consent was waived. We included consecutive patients from January 2005 to December 2014, who underwent radical cystectomy for primary bladder cancer. Cystectomy was performed by over 40 different surgeons at 5 participating institutions including 3 private hospitals and 2 public hospitals in the state of Victoria, Australia. All surgeons have performed over 20 cystectomies. The final pathological report was examined and data collected included patient age, sex, type of surgery, tumour stage, total lymph node yield, location of lymph nodes collected, number of positive nodes and location of positive nodes. Pathological stage was defined using the 2009 American Joint Committee on Cancer staging system [16]. Cystectomies for reasons other than primary bladder cancer, e.g., metastatic rectal cancer, were excluded from this study.
2. Victorian cancer registry
Subjects were followed until 31st December 2014, the last date of censoring. Mortality data was collated through a centralised government agency, the Victorian Cancer Registry (VCR) that additionally records the cause of death. The VCR is mandated by legislation to capture every cancer diagnosis in the state of Victoria. Their data record linked to our database using patient identifiers, date of birth, unique hospital identification number and date of surgery.
3. Definitions
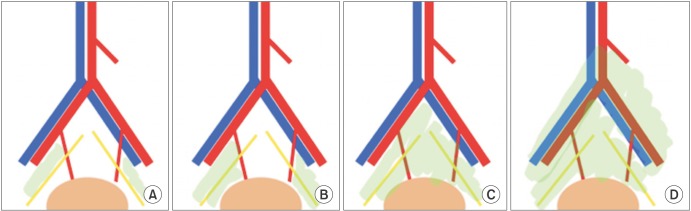
We defined “extended” surgery as a cystectomy on a female that included removal of the uterus. Extent of PLND was graded as follows: limited PLND included perivesical, pelvic not otherwise specified and obturator nodes and standard PLND (sPLND) included internal and external iliac nodes. Extended PLND (ePLND) included lymphadenectomy between the aortic bifurcation and common iliac vessels (proximally) and the genitofemoral nerve laterally. Lymph node location was defined by the pathological report which itself is derived from what the operating surgeon determined when referring the specimen. Fig. 1 highlights the varying PLND dissection templates.
4. Statistical analysis
Evaluation of the effect of LNY on bladder cancer-specific survival was undertaken by first categorising yield into 3 groups, 1 to 5, 6 to 15, and 16-plus nodes taken and generating a Kaplan-Meier plot. We then entered this variable into a multivariable Cox regression model simultaneously with sex, pathological T stage (as a 3 level categorical variable: T0/a/is/1, T2, T3/4), margin status and the continuous covariates of age at surgery and year of surgery. Additionally, we produced robust standard errors by including clustering by surgery site. Examination of Schoenfeld residuals showed that the proportional hazards assumption was not violated. Further, we examined LNY as a continuous variable in a multivariable logistic regression model with the covariates and clustering as above. The outcome was defined as death from bladder cancer within two years following cystectomy with patients alive for at least 2 years as the comparator group. Predicted probabilities for LNY were generated holding the covariates as observed. Finally, we assessed the predicted effect of node harvest in each dissection template using a multivariable logistic model including the above covariates and the number of nodes harvested in each template. Holding the covariates as observed and the node harvest at the other levels to zero generated the predicted probabilities in this model. Tests were 2 sided with significance set at 0.05 as per convention. Analyses were performed using Stata v.12 (StataCorp LP., College Station, TX, USA).
RESULTS
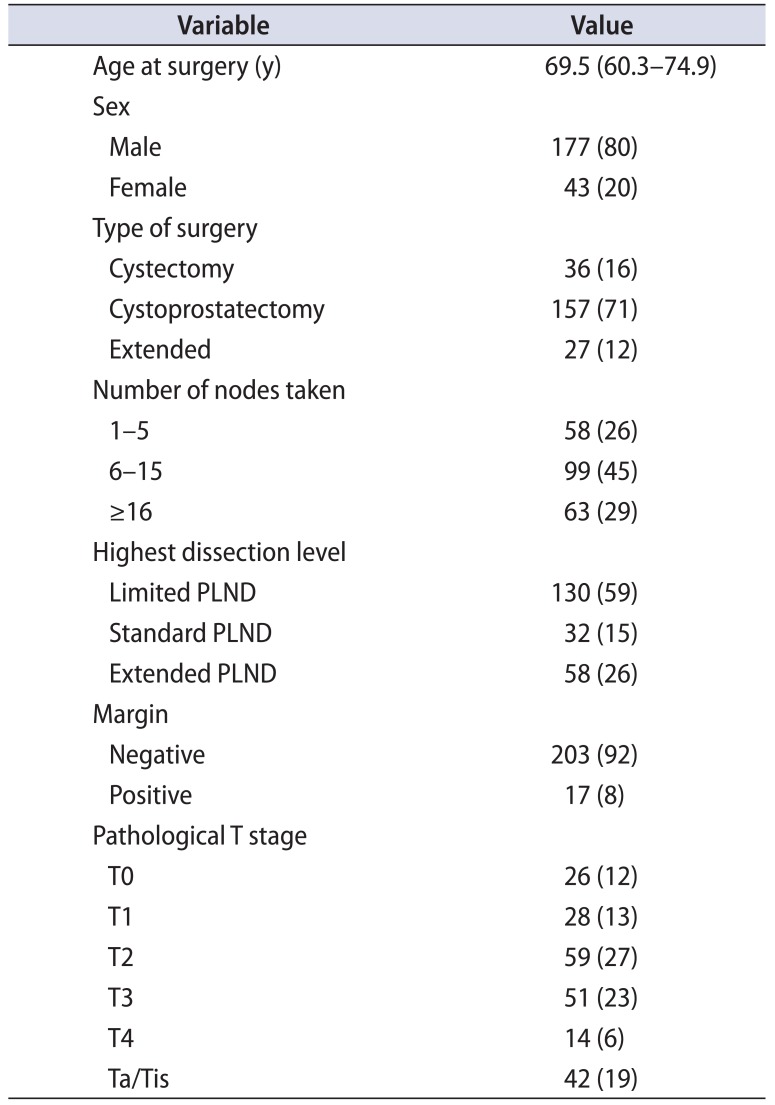
In total 353 patients were identified, of which 71 did not have any nodes taken and 62 were node positive, leaving a study cohort of 220 node-negative patients (62% of total). The greater proportion of patients were male patients (80%) and received cystoprostatectomy surgery. Of the female patients, a majority (63%) also had concurrent hysterectomy. Of the included patients, 131 recorded a time on study of 2 years or more and 55 were followed for at least 5 years. Over the entire study period, 49 (22%) suffered cancer-specific mortality, 26 of which occurred within 2 years of surgery, with a further 14 (6.4%) dying of another cause. Demographic, surgical, and pathological data are summarized in Table 1.
1. Trends in node dissection
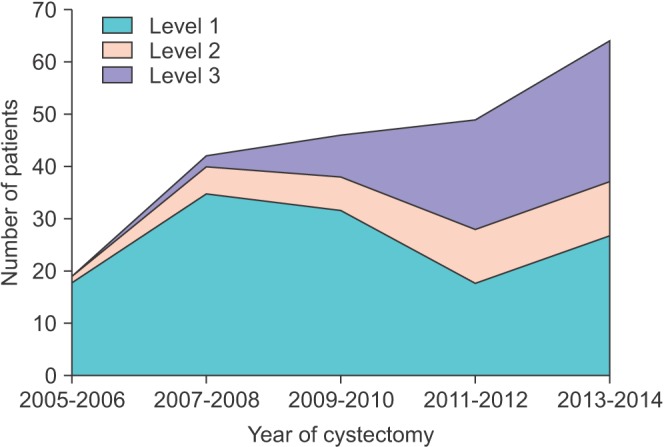
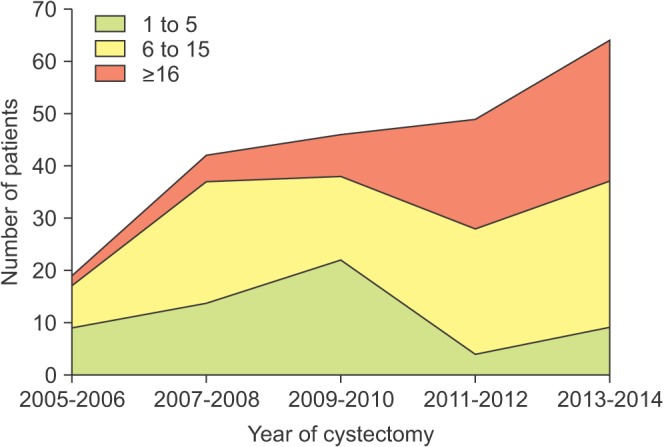
The proportion of surgeries with concomitant PLND to sPLND or ePLND steadily increased throughout the study period from 5.3% in 2005–2006 to 59% in 2013–2014 (Fig. 2). The number of nodes harvested in a cystectomy for our node-negative cohort similarly increased from a mean of 7.4 in the first 2 years to 17 in the latter 2 years (Fig. 3).
2. Effect of PLND in node-negative disease
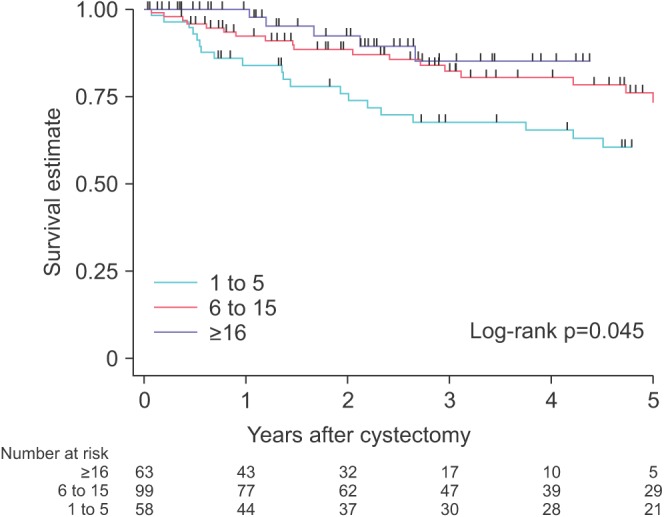
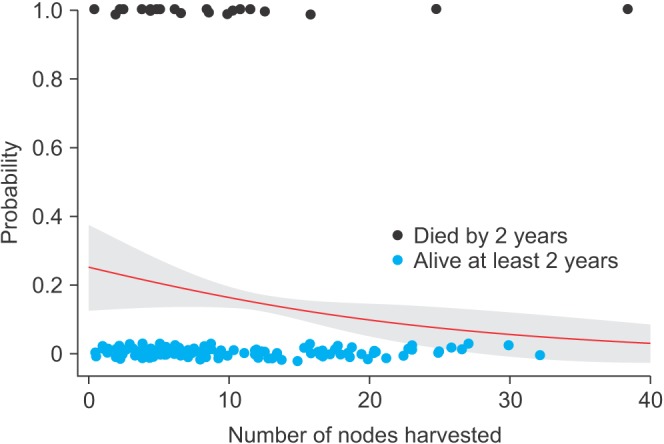
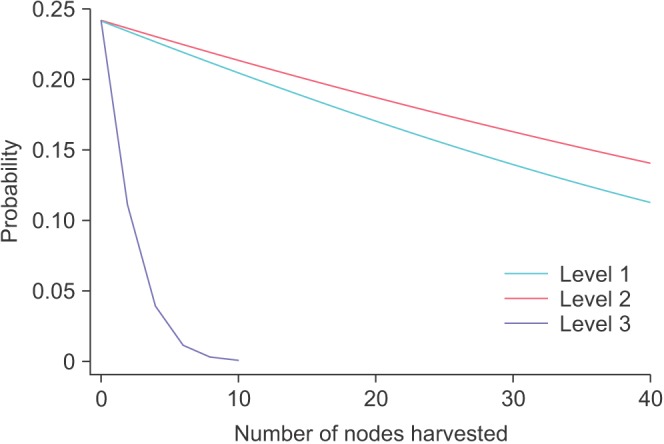
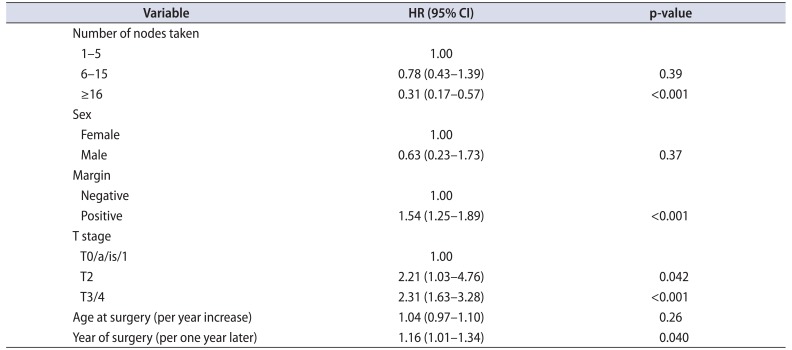
The number of nodes harvested from PLND was associated with time to cancer specific mortality. A Kaplan-Meier plot is shown in Fig. 4 with the log-rank test of overall difference between the groups reaching conventional significance (p=0.045). In a Cox proportional-hazards model with adjustment for pathological T stage, margin status, age at surgery, and year of surgery, node harvest independently predicted survival. Compared to cases where 1 to 5 nodes were taken, the hazard ratio (HR) for 6 to 15 nodes harvested was 0.78 (95% confidence interval [CI], 0.43–1.39; p=0.39) and for greater than 15 nodes the HR was 0.31 (95% CI, 0.17–0.57; p<0.001) (Table 2). Analysing node harvest as a continuous variable in a multivariable logistic model yielded a predicted probability of bladder cancer death in 2 years of 16% (95% CI, 13%–19%) for 10 nodes taken, decreasing to 5.5% (95% CI, 0%–12%) with 30 nodes taken (Fig. 5). Increasing node harvest in each dissection template was observed to decrease the chance of 2-year cancer-specific mortality (Fig. 6).
DISCUSSION
To our knowledge we present the largest Australian series investigating lymphadenectomy and disease specific survival in the surgical management of bladder cancer. The results of the current study highlight the increasing trend of aggressive node dissection in radical cystectomy patients. Further, the current study has identified improved cancer-specific survival with increased lymph node yield in nodenegative patients.
Our study identified the significant trend of increasing use of standard and extended lymph node dissection across the study period [14]. Such trends are consistent with a growing body of evidence highlighting improved oncological outcomes with more extensive lymph node dissections. Bi et al. [15] performed a meta-analysis comparing ePLND versus sPLND. Despite heterogeneity of definitions, this group defined ePLND included dissection of all lymph nodes between the aortic bifurcation and common iliac vessels (proximally), the genitofemoral nerve (laterally), and the circumflex iliac vessel (inferiorly) – consistent with ePLND in our cohort. Super-ePLND extended cranially to the level of the inferior mesenteric artery – representing a level of dissection that was not performed in our study. The pooled data analysis produced highlighted the superiority of ePLND and super-ePLND compared to sPLND, irrespective of nodal positivity status. Additionally, recent literature has directly compared the effect of ePLND and super-ePLND. Intuitively, the principles of accurate nodal staging and local cancer control would support a super extended PLND. However, such aggressive management regimes may expose patients to significant morbidity and longer operating times. Accordingly, the potential oncological benefit must be considered against to potential morbidity. Oncologically, multiple groups have reported that super-ePLND has comparable disease free survival to PLND limited to below the aortic bifurcation [1017]. Therefore, a dissection template limited to the aortic bifurcation proximally is reasonable – represented by the extended PLND cohort in our study.
Lymphadenectomy improves survival in both nodepositive and node-negative cohorts. In our cohort of nodenegative patients, we identified that increasing lymph node yield during PLND correlated with an improved oncological outcome. In the current cohort, increasing nodal harvest categorically from less than five nodes, to greater than five and greater than 15 nodes progressively improved cancer-specific survival. Our findings are corroborated by recent reports in contemporary literature [18]. May et al. [19] assessed 1,291 node-negative patients following radical cystectomy and PLND. Converse to our study, this group did not identify the continuous number of lymph nodes as significant independent predictor of cancer-specific survival (HR, 0.98; 95% CI, 0.96–1.01; p=0.140). However, utilizing a cutoff value of greater than 16 nodes resulted in a decreased probability of cancer mortality.
Further, in our cohort, improved cancer-specific survival with increased nodal yield occurred independent of dissection template. For limited, standard, or extended PLND, the risk of mortality reduced with more meticulous dissections (Fig. 5). Accordingly, it has been proposed that total lymph node yield may act as a quantitative measure of PLND quality [20]. Several groups have addressed whether a minimum number of lymph nodes should be assessed following radical cystectomy with PLND. Previous groups have proposed minimal nodal counts between 4 to 16 [9192122]. Conversely, other groups recommend thorough anatomical PLND without minimum nodal counts [11].
The precise mechanism for increased nodal yield and resulting improved survival in node-negative patients is uncertain. It is likely that in this setting, the benefit of PLND is removal of underdetected micrometastases [23]. Removal of lymph nodes with micrometastatic deposit may improve survival by reducing overall tumour burden and allowing the immune system and chemotherapeutics to target a smaller number of cancer cells [24]. New techniques employing immunohistochemical analysis and reverse transcription real-time polymerase chain reaction can aid in detection of micrometastases [2526]. It has been demonstrated that patients with micrometastases who are otherwise node-negative on routine analysis have a trend toward worse cancer specific survival and recurrence free survival than truly node-negative patients [25]. The observed predictive value of the lymph node yield may be a result of confounding patient, surgeon or institutional factors that may contribute to improved outcomes [19]. Specifically, high-risk patients may have a limited dissection while a more aggressive approach is employed in patients with superior premorbid function. Similarly, increased surgeon experience may improve quality of performing an aggressive PLND. Lastly, as highlighted by May et al. [19], this association may be the result of the Will-Rogers stage-migration phenomenon. In this setting, the examination of increased lymph nodes results in the upstaging due to more extensive nodal sampling. Accordingly, these patients are reclassified as N1 that would have otherwise been classified as N0 with high nodal yield. Subsequently, patients that underwent more extensive PLND are likely to have superior oncologic outcomes as these patients are more likely to be truly node-negative [2728].
There are several limitations to the current study. Firstly, there are inherent limitations with the retrospective nature of the current study, given data is reliant of accurate documentation. Further, several pertinent treatment details were not available for data collection. Specifically, data pertaining to neo-adjuvant, adjuvant, salvage or palliative chemotherapy or radiotherapy were not available. Our study did not assess the impact of reviewing pathologist on lymph node yield. However prior study has shown the reviewing pathologist does not alter the reported lymph node yield [29]. Despite these limitations, as highlighted, this represents the most comprehensive Australian radical cystectomy database to-date.
CONCLUSIONS
The findings of the current study highlight the increased uptake in more extensive, meticulous PLND during cystectomy for node-negative patients. Our study highlights the improved oncological outcomes with increasing LNY, irrespective of the extent of dissection. Further, robust prospective clinical research is needed to aid interpretation of lymph node dissection data.
 XML Download
XML Download