

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Interstitial cystitis (IC) is a chronic disease, characterized by varying degrees of painful and frequent urination, which likely occurs due to a variety of etiologic factors acting through multiple pathogenic mechanisms. One well-accepted hypothesis is that patients with IC can have structural and functional urothelial alterations, leading to increased bladder epithelial permeability, migration of urinary solutes into the bladder interstitium, with mast cell activation [12]. Loss of urothelial integrity can lead to neurogenic inflammation and afferent hyperactivation, with associated lower urinary tract symptoms, bladder pain and reduced bladder capacity. Although this chronic and painful condition affects up to 500 per 100,000 women, there are few effective treatment options [3]. Here we study a possible cellular pathway not previously explored for treatment.
While the cause of IC is unknown, cellular and macroscopic changes to the bladder urothelium have been characterized for many decades in patients with IC [4]. Noted urothelial changes include increased solute permeability of the urinary bladder (causing pain) and decrease of urine-bladder barrier proteins including uroplakin and unique production of Frizzled-8 protein-related glycoprotein, also known as antiproliferative factor [5]. These changes lead to disruption of the bladder lining in addition to slowing of the reparative process of the bladder wall, which is usually restored by cell replication and differentiation of basal cells [6]. Despite the use of multiple behavioral, oral and intravesical treatments for IC, efficacy rates are generally low [7].
Pentosan polysulfate is believed to augment the glycosaminoglycan layer, and to date is the only USA Food and Drug Administration (FDA)-approved oral pharmacotherapy for IC. We believe that peroxisome proliferator-activated receptor gamma (PPAR-γ) agonists may offer a potential therapeutic benefit by way of restoring the urothelial integrity. In cell culture, PPAR-γ agonists have been shown to drive urothelial cells to differentiation and production of barrier proteins including uroplakin. This differentiation persists even when other growth factors such as epidermal growth factor are inhibited [8]. PPAR- γ agonists such as pioglitazone have not been previously investigated as a potential reparative treatment for IC but may offer a treatment option that would target a known defect in urothelial architecture seen in patients with IC.
MATERIALS AND METHODS
The animal protocol was approved by the Stanford Institutional Animal Care and Use Committee (IACUC; protocol number: 30402), Sprague-Dawley female rats were purchased from Charles River Breeding Laboratories at 6 weeks of age. Animals were placed in an accredited barrier facility with targeted temperature of 22℃, and 12-hour light/dark cycles. Animals were provided food and water without restriction throughout the study protocol. Body weights of all animals were recorded on a weekly basis. Any weight loss of greater than 5% would warrant evaluation by the clinical veterinarians on site. Animal were housed in a Stanford facility accredited by the Association for the Assessment and Accreditation of Laboratory Animal Care. All methods were required to minimize pain and discomfort per the Stanford IACUC. After initial quarantine, animals were divided into 4 groups (n=6 for each group): IC plus daily sham saline gavage (IC+Pio−), IC plus daily pioglitazone gavage (IC+Pio+), normal rats with daily pioglitazone (IC−Pio+), and normal rats with neither IC nor pioglitazone (IC−Pio− or Control). Using an adaptation of prior chronic cystitis induction, animals placed in the disease groups were treated with biweekly cyclophosphamide (purity >99%, Fischer scientific labs) intraperitoneal injections (50 mg/kg) for 2 weeks (4 injections) to induce cystitis [9]. Animals placed in treatment groups were given 15 mg/kg daily pioglitazone (purity >99%, Fischer scientific) by gastric gavage [910] starting the day after the final (fourth) cyclophosphamide injection.
At the end of four weeks, terminal assays were performed to measure urinary frequency, cystometric bladder capacity and histologic evaluation of urothelial integrity. Statistical analyses were performed using Stata 13 (StataCorp., College Station, TX, USA) statistical software.
1. Physiologic voiding studies
Each rat was placed in an individual polycarbonate cage with a wire mesh floor, under which filter paper was placed to absorb voided urine. Fluid intake was restricted during this portion of the testing. Filter paper was changed every 15 minutes to avoid overlapping urine spots, and data was collected over 1 hour. Using ImageJ software, the areas of void were calculated and compared to a standard curve to determine void frequency. The standard was created using known volumes of saline dropped onto filter paper. Any volume over 0.05 mL was considered an isolated voiding event.
2. Cystometric capacity
Urethane was administered subcutaneously (1,200 mg/kg) and additional inhaled isoflurane was administered as needed (1%–4%) per IACUC recommendation. While physiologic voiding studies were accomplished in awake animals, awake urodynamics were not permitted by the IACUC, to minimize pain and suffering as well as survival surgeries. After 60 min, when no toe pinch reflex was visualized a laparotomy was then performed and the bladder was intubated through the fundus using flared polyethylene (PE)-50 tubing and 5-0 vicryl suture. Capacity was measured by incremental instillation of normal saline into the bladder at a rate of 0.1 mL/min while monitoring for leaking via the urethral meatus. Cystometric volumes were averaged over three bladder fill cycles for each rat.
3. Histology
Following completion cystometry, animals were sacrificed by isoflurane overdose. Bladders were excised then placed in 10% formalin fixative. Histologic examination was performed, after embedding the excised bladders in paraffin. Staining was completed with H&E. Slides were reviewed for bladder wall thickness and local tissue structure including urothelial cell thickness and integrity.
RESULTS
1. Body weights
All four groups (total n=24) recorded similar body weight gains, as well as gross bladder weights. Previous investigations have shown an increase in heart weight with pioglitazone treatment, but this was not investigated here [10].
2. Physiological voiding studies
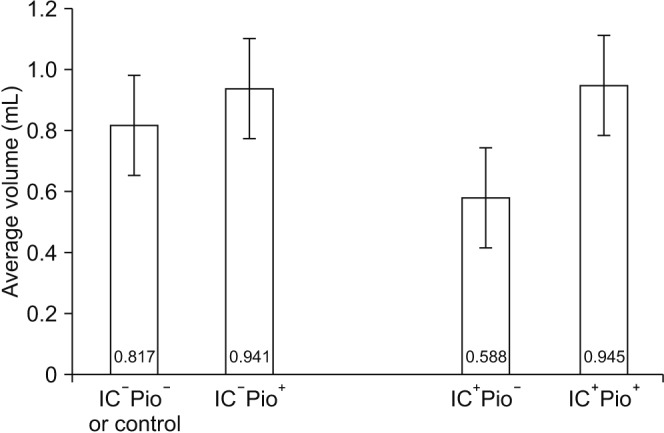
On voiding paper tests, for the rats with IC, the pioglitazone group (IC+Pio+) had statistically significantly fewer voids per hour than the IC+Pio− group (4.0±1.9 vs. 10.0±2.4, p<0.01) and had similar voids per hour when compared to control (IC−Pio−) and IC−Pio+ (Table 1). On cystometry, bladder capacity was significantly higher in IC+Pio+ versus IC+Pio− rats (0.945±0.122 mL vs. 0.588±0.165 mL:, p=0.01) (Table 1, Fig. 1). Treatment of IC rats with pioglitazone (IC+Pio+) resulted in normalization of bladder capacity, as average capacity in the IC+Pio+ group was comparable to control (IC−Pio−) and IC−Pio+ rats (Table 1).
3. Histology
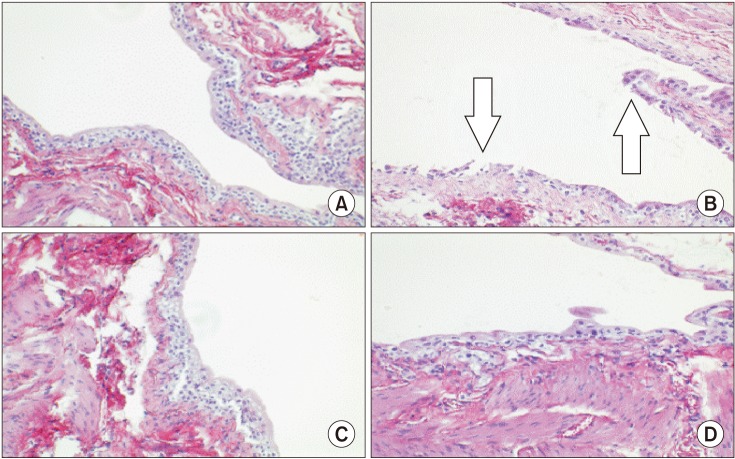
On histology, there was notable loss of urothelial integrity in IC bladders, and this effect was mitigated in the treatment group. Subjectively, no visible difference in urothelial thickness, architecture or disruptions to the bladder wall was notable in the IC−Pio+ versus the IC−Pio− group. Urothelial integrity was improved in IC+Pio+ rats versus IC+Pio− rats upon histologic observation (Fig. 2). There were no instances of urothelial or other malignancy in any treated animals.
DISCUSSION
In patients with IC, treatment responses to current pharmacological agents are generally poor. Thus, the search for alternative agents remains a goal, and pioglitazone may offer therapeutic benefit due to its action on the urothelium. As there are no obvious “curative” agents, IC is considered a chronic disease that is “managed”. Most treatments for IC are devoted to mitigation and palliation of the pain and lower urinary tract symptoms. Currently patients are treated with behavioral modifications including timed voiding and dietary modification. These interventions are often suboptimal [7]. Second-line therapy includes oral pharmacotherapy with pentosan, a daily medication that improves symptoms of IC in approximately one-third of patients, and even in that minority of positive responders, it can take 6 months to 2 years to realize therapeutic benefit [11].
Other oral agents such as hydralazine, diphenhydramine, and amitriptyline have been used off-label with varying degrees of success, yet the majority of patients do not achieve adequate symptom relief. Third-line treatment involves cystoscopy with hydrodistension of the bladder. This procedure can be both diagnostic and therapeutic, allowing the practitioner to visualize Hunner lesions and/or glomerulations, and evaluate bladder capacity under anesthesia. If Hunner lesions are present, endoscopic ablation has been shown to significantly reduce pain and urinary frequency. Unfortunately, hydrodistension and endoscopic ablation only temporizes symptoms, and typically must be repeated as frequently as every 6 to 18 months [1213]. For the typical patient, annualized cost of nonsurgical treatment was recently estimated at $3,631 using Medicare rates [1415]. In the most severe cases, the only curative procedures available to patients require extirpative surgery (removal of the bladder) and/or urinary diversion [14]. Development of a curative nonsurgical treatment for IC would help mitigate treatment cost and improve patient quality of life.
PPAR-γ agonists found original therapeutic use for patients suffering from diabetes. However, PPAR-γ receptors are found throughout the body, including the bladder [1617]. PPAR-γ agonists have been shown to drive urothelial cell differentiation, thus spurring interest for the use of these agents in the treatment of a condition where the bladder lining becomes denuded, such as IC [10]. Pioglitazone is an FDA-approved medication used for treatment of diabetes mellitus. Hypertrophy of the bladder endothelium has been demonstrated in a rat model [10]. In observational studies, a dose-dependent risk of bladder cancer has been identified in diabetics taking oral pioglitazone. While this increased risk of bladder cancer has caused the drug to be withdrawn from the market in France, recent studies have shown conflicting data, as highlighted in the recent FDA brief on pioglitazone and bladder cancer [18]. In one of the largest studies, the PROactive trial, patients were randomized to either pioglitazone or placebo for 3 years, then followed for 13 years. No increased risk of bladder cancer was revealed in this cohort [19]. In addition, a large group from Kaiser Permanente Health demonstrated a possible dose dependent increased risk of bladder cancer with prior pioglitazone use however this did not reach statistical significance [20]. Similarly, a recent meta-analysis did not show a connection between pioglitazone use and bladder cancer, with a hazard ratio of 1.07 (0.96–1.33) [21]. On the other hand, a recent meta-analysis revealed a slight increased risk of urothelial carcinoma with pioglitazone use in diabetics, prompting the FDA to recommend that pioglitazone should be avoided in patients at high risk (especially smokers) for bladder cancer [22]. We hypothesize that the same mechanism of action that may contribute to the occurrence of bladder cancer in at-risk diabetics may theoretically also allow for targeted, time-limited therapy for patients with IC, where robust cell differentiation would benefit the protective bladder layer and potentially alleviate the pain associated with Hunner lesions. While in our trial PPAR-γ agonists were only administered for 4 weeks, it is reassuring that there were no instances of urothelial or other malignancy in any of the treated animals.
Animal models help with investigations of new medications for the benefit and safety of patients. Various animal models of IC/painful bladder syndrome have been described, based upon an intervention directly affecting the bladder, upon a more systemic (inflammatory, autoimmune, or central nervous system) reaction, or using psychological or physiological stressors [23]. We chose this vesico-centric animal model due to its simplicity and low expense. Repeated low dose intraperitoneal cyclophosphamide injections elicits a chronic inflammatory process in the rat bladder, similar to the chronic nature of human IC [24].
In this study, four weeks of oral daily pioglitazone improved bladder function in rats with cyclophosphamide-induced cystitis with respect to both observed urinary frequency and measured cystometric capacity. Rat cyclophosphamide-induced cystitis causes increased voiding frequency, smaller bladder capacity, and disruption of the urothelial lining. This urothelial disruption is present in patients with IC and Hunner lesions, manifesting histologically as areas of severe urothelial denudation, and macroscopically as ulcers [25]. While no animal model completely predicts human response, we demonstrated improvement in all the above surrogate assays, lending legitimacy to the possibility of a future treatment for patients using PPAR-γ agonists.
To date, this is the first study to address possible treatment of IC with a PPAR-γ agonist. The study reliably demonstrated changes in the rat bladder physiology, providing the foundation for future studies regarding a potential benefit to patients. Future studies may answer if alternative routes of administration may provide an improved risk/benefit profile. For example, bladder instillation of pioglitazone metabolites may create a therapeutic effect and minimize systemic side effects. Similarly, our study showed that pioglitazone appears to restore urothelial integrity in rats with cyclophosphamide induced bladder injury. The current study is limited as only the feasibility of an oral dose treatment was tested in an established animal model of disease. Our very limited budget did not allow for the participation of a pathologist trained in rat bladder pathology. Perhaps in a future study, we will be able to more systematically evaluate the bladder histology and quantify it using a qualified pathologist, a larger number of animals, and a standardized histological evaluation. Additional investigation including cytokeratin staining and investigation into the bladder surface protein changes may better illuminate structural bladder changes with treatment, and measurement of transepithelial resistance or measurement of diffusion of tritiated urea across the membrane could objectively evaluate urothelial barrier function. However, this was not possible with the current investigation. Moving from animal to human investigation would also provide more compelling evidence for future therapeutic use. An additional limitation of this treatment is the potential risk of bladder cancer with chronic pioglitazone treatment. This is particularly concerning, as IC is a chronic disease, that may respond better to chronic rather than time-limited therapy. Obviously upon translation to human studies, investigation must determine if short-term or intermittent PPAR-γ agonist treatment will suffice for repair of any contributory urothelial dysfunction, or if chronic therapy is needed to prevent relapse. Vigilance will certainly be necessary regarding the development of urothelial carcinoma if chronic administration is required.
In summary, while concern remains regarding a potential (but unconfirmed) risk of bladder cancer in diabetics who use pioglitazone, pioglitazone and other PPAR-γ agonists, due to their propensity to cause bladder urothelium differentiation, may prove to be useful for treating IC, and deserve further study.
CONCLUSIONS
In a cyclophosphamide-induced cystitis model of IC pioglitazone, a PPAR-γ agonist, improved bladder function. Cystometric capacity and urinary frequency, which were higher rats with cystitis, were normalized following treatment with pioglitazone. In addition, the structural integrity of the urothelial was improved. And while concern remains for the potential increase in urothelial carcinoma with long-term PPAR-γ agonist treatment, pioglitazone, due to a propensity to cause bladder mucosal proliferation, may prove useful for treating IC, and deserves further investigation.

 XML Download
XML Download