

 PDF
PDF Citation
Citation Print
Print



Introduction
Antiplatelet therapy has become the cornerstone of clinical management of acute coronary syndrome (ACS). There has been extensive research into both physiological and pathological roles that platelets play in hemostasis and thrombosis for more than half a century. Antithrombotic properties of aspirin were recognized as early as in the 1950's [1], but aspirin's cardioprotective effects were confirmed merely two decades ago [2]. The development of percutaneous coronary intervention (PCI) was the driving force behind the evolution of antiplatelet regimen as a prevention for early stent thrombosis. Different classes of antiplatelet agents have been introduced since late 1990's, which include the glycoprotein IIb/IIIa (GPIIb/IIIa) receptor antagonists, and thienopyridine derivatives [34]. A method to evaluate platelet function was originally described by Professor Born [5] in the form of a light transmission platelet aggregometry in the 1960's. However, platelet function testing was not widely adopted in monitoring antiplatelet therapies until a simple whole blood test format became available [6]. The importance of platelet function testing has drawn more attention after high ontreatment platelet reactivity (HPR) was reported to increase major adverse cardiac events (MACE) after PCI [78]. Conversely, extremely decreased (low on-treatment) platelet activity upon testing may be regarded as an increased risk for bleeding complications [910], therefore dosing of the respective agents needs to be carefully adjusted in patients at high risk for bleeding.
Today, physicians are required to manage complex coagulation problems of critically ill patients, and therefore understanding of current antiplatelet agents, hemostasis monitoring and therapeutic strategies is quite important. The aims of this article are to review the role of dual antiplatelet therapy, and to discuss clinical implications of platelet function testing in preventing thrombosis and hemorrhage in the perioperative setting.
Platelet Inhibitors and Cardiac Surgery
Aspirin
The majority of patients with coronary artery disease (CAD) or peripheral vascular disease take aspirin for primary or secondary prevention of thrombotic events. Aspirin (acetylsalicylic acid) exerts its antiplatelet activity via rapid-irreversible inhibition of the cyclooxygenase-1 enzyme [11], inhibiting the conversion of arachidonic acid to thromboxane A2 (TXA2). Platelet aggregation via the thromboxane-prostanoid (TP) receptor is thus inhibited after aspirin ingestion. Because thromboxane expression is increased during inflammatory states (e.g., surgery), aspirin has the potential to decrease platelet aggregation during the perioperative period. Aspirin may be beneficial as an antiinflammatory and antithrombotic agent, but it may also increase the risk of bleeding.
There is mixed evidence about whether to withhold aspirin during the perioperative period in patients with cardiovascular disease. Potential reasons to continue aspirin are prevention of perioperative myocardial ischemia, stent thrombosis, and stroke. However, in the POISE-2 trial (Perioperative Ischemic Evaluation-2; NCT01082874) continuation of aspirin during the perioperative period did not decrease the risk of stroke or myocardial infarction (MI) in “non-cardiac” surgical patients. The main argument for withholding aspirin is to decrease major bleeding, which appeared to increase in the aspirin versus the placebo cohort (hazard ratio 1.23; 95% CI 1.01–1.49) according to the POISE-2. However, aspirin was not reported to increase perioperative bleeding in several large observational studies involving cardiac surgical patients receiving aspirin before or early after surgery [1213]. In a recent prospective randomized controlled trial of coronary artery bypass surgery (CABG) patients, aspirin was not associated with increased bleeding [14]. Further, perioperative aspirin use may be beneficial in cardiac surgery, decreasing complications such as MI and renal failure after surgery [121315]. Aspirin may even confer a lung protective effect after massive transfusion after cardiac surgery as reported in one observational study [16].
Lack of aspirin-associated bleeding in contemporary cardiac surgical patients may be due to the ubiquitous use of antifibrinolytics. In a large randomized controlled trial of tranexamic acid (TA) in CABG patients, the risk for major bleeding was decreased by approximately 50% with TA [17]. Taken together, patients are likely to be continued on aspirin through most of the perioperative period due to lack of higher level evidence to withhold it before cardiovascular surgery.
P2Y12 inhibitors
In the early 1990s, aspirin was used in conjunction with heparin or warfarin after bare-metal coronary stent placement, but the stent thrombosis rate was still 3.5%, and bleeding complications were not uncommon [18]. Dual antiplatelet therapy (DAPT) using aspirin and ticlopidine, a thienopyridine P2Y12 inhibitor, was introduced, decreasing the rate of stent thrombosis to about 1% [4]. The 2nd generation thienopyridine, clopidogrel is now widely used in the setting of ACS and PCI [19]. Activation of P2Y12 receptor is crucial in sustained platelet aggregation induced by adenosine diphosphate (ADP) at the vascular injury site [20].
The introduction of drug-eluting stents (DES) reduced instent restenosis by inhibiting neointimal hyperplasia, but the risk of stent thrombosis remained high due to delayed re-endothelialization. Minimum duration of DAPT is an evolving concept, but at least 6 and 12 months of DAPT are recommended after DES placement for stable CAD and ACS, respectively according to the 2016 update of the ACC/AHA guideline [21]. In the case of high-risk bleeders, durations may be shortened to 3 and 6 months in stable CAD and ACS, respectively [2122]. Aspirin monotherapy is generally sufficient for elective CABG patients with stable CAD, but 6–12 months of DAPT are recommended for CABG patients with recent ACS and/or PCI [21].
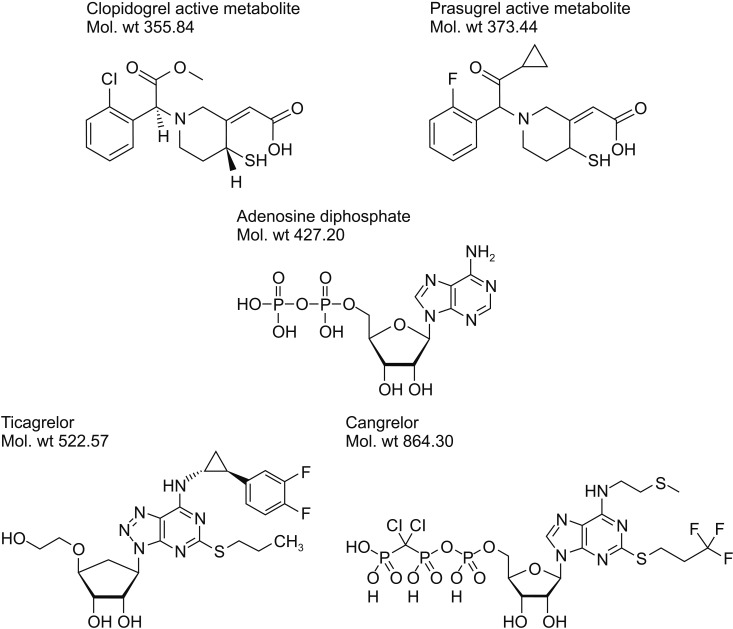
Currently available P2Y12 platelet inhibitors are shown (Fig. 1). Clopidogrel is a widedly used thienopyridine prodrug, which undergoes 2-step hepatic metabolism involving cytochrome P450 (CYP). Its antiplatelet activity may be influenced by polymorphisms of CYP2C19. A higher incidence of poor metabolizers in Korean and Japanese populations has been reported than elsewhere [23]. The genotypes CYP2C19*2 and CYP2C19*3 represent a “slow metabolizer” of clopidogrel or “non-responder.” HPR is in part attributed to gene polymorphisms, which appear to increase the rate of MACE while on aspirin and clopidogrel after DES implantation [24].
The 3rd generaiton thienopyridine, prasugrel is also a prodrug, but is rapidly activated via single CYP450-mediated oxidation [25]. Prasugrel is thus presumed to be less prone to CYP polymorphisms, and have more predictablle pharmacokinetics. Efficacy and safety of prasugrel were compared with clopidogrel in moderate-high risk ACS patients undergoing PCI (n = 3,534) in TRITON-TIMI 38 (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition With Prasugrel-Thrombolysis In Myocardial Infarction 38; NCT00097591) [26]. Prasugrel was associated with decreased risk of 30-day MACE compared to clopidogrel (6.5% vs. 9.5%) (hazard ratio 0.69; 95% CI 0.54–0.87; P = 0.0017). Less than 4% of studied patients underwent CABG, but TIMI major bleeding1) after CABG was reported more frequently in the prasugrel group (12 of 64; 18.8%) than in the clopidogrel group (2 of 73; 2.7%) (odds ratio 8.19; 95% CI 1.76–38.18; P = 0.0033) [26].
Platelet transfusion was more frequent in the prasugrel group, but only trends for increased transfusion of packed red blood cells (PRBC) and plasma were observed. The timing of stopping thienopyridines was shown to be important in this study. When prasugrel was stopped more than 7 days before CABG, postoperative blood loss and transfusion requirements were similar to the clopidogrel group [27]. It is possible that hemorrhagic side effect of prasugrel may be modulated by dose adjustment in patients at high risk for bleeding. In PRASFIT-ACS (Prasugrel compared with clopidogrel for Japanese patients with ACS undergoing PCI), one-third dose of prasugrel that is used in United States/Europe was evaluated against the standard dose of clopidogrel (Table 1) [28]. The incidence of MACE was numerically lower with prasugrel compared to clopidogrel, although the difference was not statistically significant (9.4% vs. 11.8%; hazard ratio 0.77; 95% CI 0.56–1.07). The incidence of the composite of major, minor, and clinically-relevant bleeding was 9.6% in both prasugrel and clopidogrel groups [29]. In the whole cohort (n = 1,363), pharmacodynamics of prasugrel (i.e., extent of platelet inhibition) was not found to be a bleeding risk factor. The key bleeding risk factors were female gender, low body weight (≤ 50 kg), advanced age (≥ 75-year-old), and diabetes mellitus in this Japanese cohort [29].
Ticagrelor is a cyclopentyl-triazolo-pyrimidine, which reversibly inhibits P2Y12 receptors in contrast to the covalent bond formation between thienopyridines and ADP binding sites [30]. A lower risk of bleeding was initially anticipated for ticagrelor, but no difference in the risk of CABG-related bleeding was demonstrated between ticagrelor and clopidogrel groups in the prospective randomized PLATO trial (Platelet Inhibition and Patient Outcomes; NCT00391872) involving 18,624 patients [31]. Within the ticagrelor group, a significantly higher risk of CABG-related bleeding was recognized when the time of surgery was less than 72 h from drug discontinuation [32]. The odds ratio of bleeding was 5-fold increased in this cohort when compared to 2 cohorts with 72–120 h and >120 h of discontinuation. Major bleeding was more common with both ticagrelor and clopidogrel when drug discontinuation was within 24 h of CABG; the incidences of bleeding were 38% and 31%, respectively according to the BARC-CABG definition [33].2)
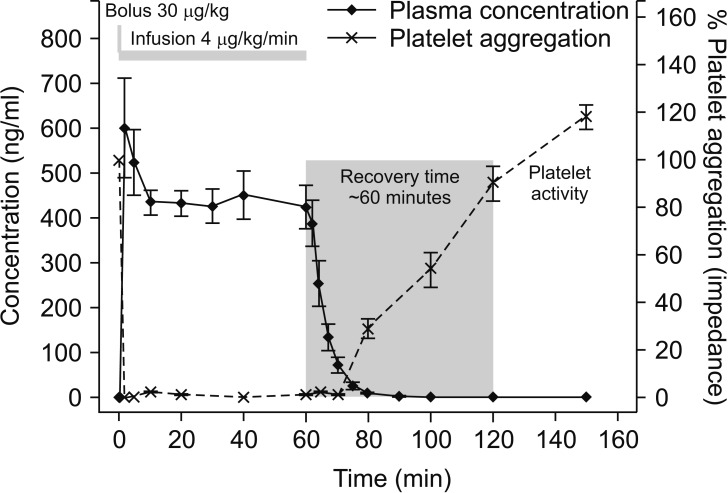
Cangrelor is a non-thienopyridine and modified ADP derivative with an extremely short half-life (3–6 min) [3435]. Platelet inhibition (> 80%) is rapidly achieved after a loading dose of 30 µg/kg followed by 4 µg/kg/min infusion, while a full recovery of platelet function is observed in ~60 min of drug discontinuation (Fig. 2) [36]. The CHAMPION-PHOENIX trial (Cangrelor versus Standard Therapy to Achieve Optimal Management of Platelet Inhibition; NCT01156571) is a comparison of cangrelor and clopidogrel (n = 11,145) in the ACS setting, which reported that stent thrombosis was developed in 0.8% and 1.4%, respectively (odds ratio 0.62; 95% CI 0.43–0.90; P = 0.005) [37]. The major side effect of cangrelor is a transient dyspnea, which occurred in 1.2% of cangrelor-treated subjects. Utility of cangrelor in a transition from thienopyridines to major cardiac surgery was tested in the BRIDGE trial in which cangrelor or placebo was infused up to 7 days before CABG [38]. Cangrelor was stopped 1–6 h before surgery, and there was no significant difference in CABG-related major bleeding between placebo and cangrelor (10.4% vs. 11.8%). Preoperative platelet inhibition (> 60%) in the cangrelor group did not lead to a statistically significant reduction in ischemic events (2.8% vs. placebo 4.0%). Minor bleeding incidences were more frequent in the cangrelor group before surgery, but there was no significant difference from the placebo in terms of major bleeding events.
Taken together, various P2Y12 inhibitor agents are being utilized extensively in high-risk CAD patients who might present to elective and urgent cardiovascular surgery. It is crucial to understand differences in pharmakinetics and pharmacodynamics among different P2Y12 inhibitors, so that perioperative risks of ischemia, stent thrombosis, and bleeding can be minimized.
Platelet Function Tests
Variability in response to antiplatelet agents, and non-compliance raise the importance of testing platelet function in patients on DAPT. Light transmission aggregometry (LTA) in platelet-rich plasma has been the gold standard in platelet function testing. However, LTA is technically cumbersome, and time-consuming, and therefore it was not widely utilized in the perioperative setting beyond the assessment of congenital platelet disorders [39]. In the recent years, several whole blood platelet function tests have become commercially available, and some are used as a point-of-care (POC) test. However, each device has different features including sample processing, type and potency of platelet agonists, and method of detecting platelet activity [40]. In the following section, key features and clinical utilities of several POC devices will be discussed.
The VerifyNow® system (Accriva Diagnostics, San Diego, CA, USA) has been extensively studied in clinical trials involving P2Y12 inhibitors in the North America [41]. P2Y12 reaction unit (PRU) is automatically measured in citrated whole blood mixed with a lyophilized ADP (20 µM), prostaglandin E1 (PGE1; 22 nM) and fibrinogen-coated polystyrene beads. Agglutination between activated platelets and fibrinogen-coated beads causes an increase in light transmission, which is used to calculate “PRU.” The presence of PGE1 elevates intra-platelet cyclic adenosine monophosphate, making platelet activation more dependent on P2Y12 activation. Normal PRU is reported in the range of 180–376, and P2Y12 inhibition is assumed for PRU below 180. HPR was defined as PRU above 208 on clopidogrel in a prospective randomized study involving stable CAD with at least 1 coronary stent (n = 423), comparing prasugrel 10 mg versus clopidogrel 75 mg daily. After 3 months of intervention, PRU (median, interquartile range) decreased from 245 (225–273) to 80 (42–124) in 212 patients who were switched to prasugrel, while PRU values were 241 (194–275) in 211 patients who remained on clopidogrel. The primary endpoint of cardiac death or myocardial infarction at 6 months occurred in very few patients, and thus clinical implication of HPR was not demonstrated. During 6 months period, major bleeding occurred in 3 patients (1.4%) on prasugrel, and 1 patient (0.5%) on clopidogrel. As mentioned, low-dose regimen of prasugrel was tested in Japan in ACS patients undergoing PCI, and it was non-inferior to the standard dose of clopidogrel (Table 1). The prevalence of HPR (PRU > 208) was reduced after switching to prasugrel from clopidogrel in a subset (n = 53) of slow metabolizers (CYP2C19*2/CYP2C19*3) [42]. Baseline PRU values (mean ± SD) were similar in the prasugrel and clopidogrel groups (231 ± 57 vs. 237 ± 58, P = 0.65). PRU values were lower with prasugrel than clopidogrel at 24 h (147 ± 80 vs. 261 ± 57, P < 0.001), and in 2 weeks (171 ± 67 vs. 221 ± 70, P = 0.005). No specific threshold PRU values predictive of non-CABG major bleeding events were found, but bleeding risks were associated with females, low body weight (≤ 50 kg), advanced age (≥ 75-year-old), and diabetes mellitus [29].
VerifyNow® system can be thus used to assess pre-procedural P2Y12 blockade [43]. However, its intra- and post-operative uses can be hindered by low hematocrit, which spuriously increase PRU values [44].
The Multiplate® system (Roche Diagnostics, Rotkreuz, Switzeland) is a whole blood impedance aggregometry commonly used in cardiology and perioperative settings in Europe. Whole blood is collected in a hirudin tube, and each sample (300 µl) is mixed with normal saline (300 µl) in a test well containing 2 independent sensor units (electrode wires). For P2Y12 testing, ADP (6.4 µM) is added as an agonist, and electrical impedance changes are monitored while activated platelets adhere to the electrodes. Impedance changes in 2 sensor units are traced for 6 min, which are averaged to calculate area under the curve (AU x min). One Multiplate® unit (U) is defined as 10 AU x min, and normal ADP response is 57–113 U. In a PCI study involving 2,533 patients receiving a loading dose of clopidogrel (600 mg), Multiplate® ADP test value below 19 U (n = 975) was associated with a 2.6-fold higher major bleeding risk after PCI [45]. In the surgical setting, there is a paucity of data on the optimal threshold on Multiplate® ADP test that might predict increased bleeding and platelet transfusion. In a single-center study involving 87 patients on ticlopidine or clopidogrel, ADP test below 31 U before surgery was reported as an optimal cut-off (sensitivity 72%, specificity 66%) for increased bleeding (> 800 ml in 12 h). However, the size of bleeding cohort was small (n = 14), and intra/post-operative ADP results were not included. A larger clinical study is warranted to validate the role of intra/post-operative monitoring of ADP response [4647].
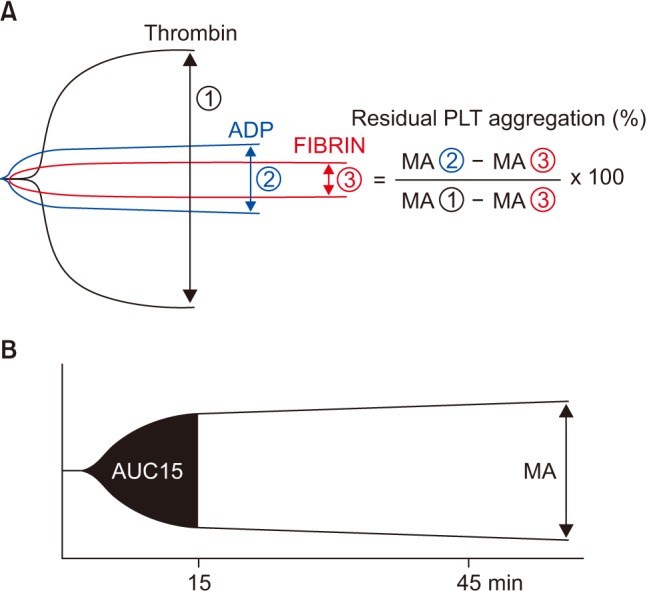
TEG® Platelet Mapping™ (Haemonetics, Braintree, MA, USA) is the thrombelastography-based platelet function test for monitoring aspirin or P2Y12 inhibitors. For P2Y12 inhibitior assay, heparinized whole blood is mixed with ADP (2 µM) and Activator F™ (reptilase and activated FXIII), which separately trigger platelet activation and fibrin polymerization, respectively. ADP-stimulated maximum amplitude (MAADP) and fibrinspecific MA (MAFib) are used to calculate platelet inhibition in reference to thrombin-mediated MA (MAThrombin) using the standard kaolin TEG® (Fig. 3A) as follows;
Alternatively, area under the curve of ADP-stimulated TEG® waveform at 15 min (AUC15) is used for a faster result (short TEG®) (Fig. 3B) [4849]. HPR during clopidogrel therapy is defined as < 30% decrease in AUC15 in the ADP channel relative to the kaolin channel [48].
In one preoperative platelet assessment study involving clopidogrel-treated and untreated patients, the mean MAADP in the clopidogrel group was lower, but there was a significant overlap in the calculated % platelet inhibition between the control (47.8 ± 18.9%) and clopidogrel treatment (71.5 ± 18.4%) [50]. This non-specificity may be attributed to a lower ADP concentration used in the Platelet Mapping™ assay, and its % inhibiton cannot be generalized to other platelet function tests.
Stratifying CABG patients to a specific waiting period based on the MAADP (3–5 days for 35–50 mm, and > 5 days for < 35 mm) was previously evaluated in the clopidogrel-treated (n = 86) and untreated control patients (n = 94) [51]. The average waiting was reduced by 46% to 2.7 days versus the standard 5 days in the clopidogrel group, and similar PRBC transfusion rate and postoperative bleeding were reported between 2 groups [51]. Intra/post-operative uses of Platelet Mapping™ may be hindered by fluctuating fibrinogen and hematocrit levels.
In summary, POC assessment of platelet P2Y12 function has become feasible, and useful in optimizing the timing of surgery, but the results from different tests are not interchangeable. Further, evidence that supports intraoperative platelet function testing is rather limited for the predictions of bleeding, and need for platelet transfusion.
Effects of Cardiopulmonary Bypass on Platelet Function Tests
Use of cardiopulmonary bypass (CPB) affects platelet count and function in multiple ways. To name a few, heparin, protamine, and hypothermia modulate platelet activity [525354]. Sequestration of platelets in the spleen and liver occurs under hypothermia [55], and thrombocytopenia resulting from hemodilution (crystalloid or colloid solution) is not uncommon [56].
Assessment of platelet function before and after CPB using LTA and multiple electrode aggregometry has demonstrated that the platelet responses to TXA2 and ADP are decreased immediately after CPB regardless of the status of preoperative platelet inhibition, or adjustments of platelet counts in test samples (as performed in LTA) [475758]. These data indicate that platelet surface TP and/or ADP receptors are temporarily less responsive to agonist stimulation when hemostasis needs to be established after CPB. Postoperatively platelet function appears to recover gradually after 3 h, and returns to normal in 24 h [5758].
Whole blood platelet function tests obtained after CPB often demonstrate abnormal aggregation patterns using various agonists on Multiplate®, TEG® Platelet Mapping™ or Plateletworks® (Helena, Beaumont, TX, USA) [4647596061]. Only a portion of those who demonstrate a below-normal platelet function require actual platelet transfusion [4659].
Testing platelet function as routine part of transfusion algorithm remains controversial. Intraoperative POC use of Multiplate® did not result in statistically significant reduction in platelet transfusion, but ROTEM® use effectively reduced plasma transfusion in 100 cardiac surgical patients randomized to conventional care or POC-based management [46].
Conversely, in a large scale prospective before-and-after trial (stepped-wedge clustered randomized study) involving 7,402 patients, relative risks of PRBC transfusion, and platelet transfusion were reduced after the POC implementation (ROTEM® and Plateletworks®; n = 3,847); adjusted relative risk 0.91 (95% CI 0.85–0.98; P = 0.02) for PRBC, and relative risk 0.77 (95% CI, 0.68–0.87; P < 0.001) for platelets [62]. There was noticeable variability in blood product usage among 12 study sites, and POC testing did not reduce plasma usage. Indeed, transfusions of platelets and plasma occurred in up to 40% of patients at some sites even after POC implementation.
Platelet Transfusion and Adjunct Therapies
There is a paucity of data on the clinical efficacy of allogeneic platelet transfusion, particularly for the reversal of P2Y12 inhibitors. In vitro platelet supplementation experiments previously demonstrated that the functional platelet recovery was minimal when freshly prepared platelet concentrate (equivalent to 3–4 apheresis units) was added to the sample blood obtained in 2 h after the dosing of prasugrel [63] or ticagrelor [64] in addition to aspirin. The half-lives of active metabolites of prasugrel and ticagrelor are approximately 8 h (Table 2) [2530], and thus transfused platelets are also susceptible to P2Y12 inhibition during this interval. On the contrary, > 80% of normal platelet activity was recovered when the fresh platelet concentrate was supplemented in vitro to blood samples from the subjects whose last doses of clopidogrel and aspirin were 24 h prior [65].
The age of platelet concentrates is an important consideration in the reversal of P2Y12 inhibitors in clinical practice. During the storage period of 5 days, platelet aggregation to ADP (5 µM) was decreased from 60–70% at baseline to 24–30% by day 3, and 13–25% by day 5 using 3 different commercial platelet storage bags [66]. Indeed, transfusion of 3-day-old autologous apheresis platelets (2 units) in the subjects who received 3-day course of aspirin plus clopidogrel did not normalize ADP (20 µM)-induced platelet aggregation on LTA, but only restored it to 31–38% (normal, 70%) in 24 h [67].
Severe bleeding diathesis refractory to multiple platelet transfusions had been reported after urgent/emergent cardiovascular surgery involving patients who were receiving a potent P2Y12 inhibitor [68]. When faced with emergency surgery in patients on P2Y12 inhibitors, adjunct hemostatic therapies may be necessary to mitigate postoperative hemorrhage refractory to platelet transfusion. Recombinant activated factor VII (rFVIIa, NovoSeven®, Bagsbaerd, Denmark) was once touted and used as a “universal hemostastic agent” in many bleeding conditions including post-CPB coagulopathy [69]. Although it may be efficacious, this type of off-label use has been associated with serious thrombotic complications, particularly in the elderly [70]. In a small study involving healthy volunteers who had therapeutic effects of clopidogrel (300 mg, followed by 75 mg for 2 days), 10 and 20 µg/kg of rFVIIa (n = 6 and 12) were shown to reduce the bleeding volume from a standardized punch biopsy wound compared to the placebo (n = 13) [71]. This finding is a proof of concept, but efficacy and safety of rFVIIa cannot be extended to cardiac surgical patients who develop multi-factorial coagulopathy in addition to platelet P2Y12 inhibition. In a prospective placebo-controlled cardiac surgical study of rFVIIa, bleeding post-CPB patients were randomized to the placebo (n = 68), 40 µg/kg (n = 35) or 80 µg/kg of rFVIIa (n = 69). The safety end points of this study indicated that death and cerebral infarction were increased in the rFVIIa cohorts relative to the placebo (odds ratio 1.67; 95% CI 0.50–5.47), although re-exploration and allogeneic transfusion rates were reduced by rFVIIa [72]. Advanced age (≥ 75-year-old) is an important risk factor for both P2Y12 inhibitor related bleeding [29], but it is also associated with rFVIIa-related thrombosis [70]. It is thus important to carefully consider the risk/benefit ratio of these interventions in the elderly.
Desmopressin (d-arginine vasopressin; DDAVP) is a therapeutic agent that is indicated for certain types of von Willebrand disease (vWD) (type 1 and type 2a) [73], and mild hemophilia A [74]. Clinical evidence for the efficacy of DDAVP is rather poor [70], particularly for the reversal of P2Y12 inhibitors. However, the drug is relatively safe with few serious side effects reported [75]. Plasma levels of high-molecular-weight von Willebrand factor (vWF) multimers are increased from 116% to 160% (interquartile range 102–154%) with 0.3 µg/kg of DDAVP in post-CPB patients without vWD [76]. However, increased vWF levels may not translate into stable thrombus formation in patients on P2Y12 inhibitors [76].
Antifibrinolytic Therapy and P2Y12 inhibitors
Antifibrinolytic therapy has become ubiquitous in cardiac surgical patients, and is currently a Class 1a recommendation in the 2012 STS/SCA3) guideline [77]. However, it remains unclear to what degree antifibrinolytics (ε-aminocaproic acid or TA) can mitigate hemorrhagic side effects of potent ADP inhibitors such as clopidogrel, prasugrel, and ticagrelor. In one randomized controlled trial that included 570 CABG patients, 10 mg/kg bolus of TA, followed by an infusion of 10 mg/kg/h reduced blood loss when compared to controls that did not receive TA. This study suggested that TA's beneficial effects were greater in patients who received clopidogrel within 7 days of surgery, meaning there was more reduction in blood loss in this group. These findings associated with TA in clopidogrel-treated patients cannot be simply inferred to patients on prasugrel and ticagrelor as more extensive P2Y12 inhibitions than clopidogrel are generally observed [6478]. Further, high doses of TA (30 mg/kg then 10–16 mg/kg/h) [79] may increase the incidence of postoperative seizure [80], and thus dose escalation of TA should be cautioned in patients on P2Y12 inhibitions.
Conclusions
The recent advances in the stent designs/materials, and placement techniques have significantly reduced the incidences of MACE after PCI [81], and it may be possible to further shorten the duration of DAPT after DES implantation in the future [82]. Stent thrombosis is one of the most feared perioperative complication, and it is important to optimize the care of high-risk patients by utilizing various antiplatelet agents with different pharmacokinetics and pharmacodynamics. Routine platelet function testing in every cardiac surgical case is not warranted, but POC platelet function tests are useful in confirming residual P2Y12 inhibition, and adjusting a waiting period before surgery [4351].
Further inter-disciplinary research efforts are needed: 1) to better stratify patients at high risk for perioperative thrombosis and/or bleeding, 2) to standardize perioperative monitoring of antithrombotic therapies, and 3) to assess multi-modal hemostatic approaches to bleeding secondary to antiplatelet therapy.
 XML Download
XML Download