

 PDF
PDF Citation
Citation Print
Print


Introduction
Traditionally, train-of-four (TOF) stimulation at adductor pollicis muscle has been used in research and clinical practice. The muscle is easily accessible and essential for determination of recovery of neuromuscular transmission after neuromuscular blockade [1,2]. The use of the dominant hand may cause increased mechanical activity of the motor units in the dominant muscles in electromyographic studies [3]. A different sensitivity in the response to vecuronium in the dominant compared to the nondominant extremity [4]. However, Michaud et al. [5] contradicted these results showing no difference in onset time, maximum effect, single twitch, and TOF ratio between either adductor pollicis muscle using phonomyography. Despite the fact that phonomyography is a relative new method for recording neuromuscular blockade with high sensitivity and applicability at most superficial muscles, slight movements of the microphone relative to the skin during surgery and movement of the arm could lead to a significant bias [6].
The present study was aimed at investigating the influence of hand dominance on measurements of neuromuscular blockade at the adductor pollicis muscle using acceleromyography.
Materials and Methods
This clinical observation study was approved by the Hospital Ethics Committee. Written informed consent was obtained from all patients. In total, 31 patients, aged 23 to 58 years, with an American Society of Anesthesiologists physical status of I or II and undergoing elective surgery with a general anesthesia in the supine position were studied. Exclusion criteria included body weight 20% greater than ideal body weight, a pregnancy, patients with neuromuscular, hepatic, or renal diseases, and patients receiving medications known to interact with neuromuscular blockade.
No premedication was given. After arrival to the operating room, electrocardiography, non-invasive measurement of blood pressure and oxygen saturation were performed. All patients were connected to a bispectral index (BIS) monitor (Model A 2000, Aspect Medical Systems, Natick, MA, USA). Anesthesia was induced with remifentanil 0.5 µg/kg/min injected intravenously over 2 minutes (min) followed by propofol 2.0-2.5 mg/kg injected intravenously over 30 seconds (s). After loss of consciousness, ventilation via facemask with a fresh gas flow at 4 L/min (50% nitrous oxide in oxygen) was controlled manually to maintain the end-tidal CO2 at 30 to 35 mmHg. Maintenance of anesthesia was with 1.0-1.5 MAC of sevoflurane in a gas mixture of 50% nitrous oxide in oxygen to maintain a BIS between 40 and 50 and infusion doses of remifentanil 0.05-0.20 µg/kg/min throughout surgery.
Neuromuscular function was assessed using acceleromyography of the adductor pollicis muscle (TOF-Watch SX®, Organon Ltd., Dublin, Ireland). Before placing the surface electrodes, the skin overlying the ulnar nerve of the dominant and nondominant hands was cleansed with isopropyl alcohol. Two electrodes (Cleartrode™, Ref 1720-003, ConMed®, Utica, NY, USA) were placed over the prepared skin on both forearms. A force transducer was fixed to the thumb. No special arm board was used and no preload was applied to the thumb during the entire study procedure.
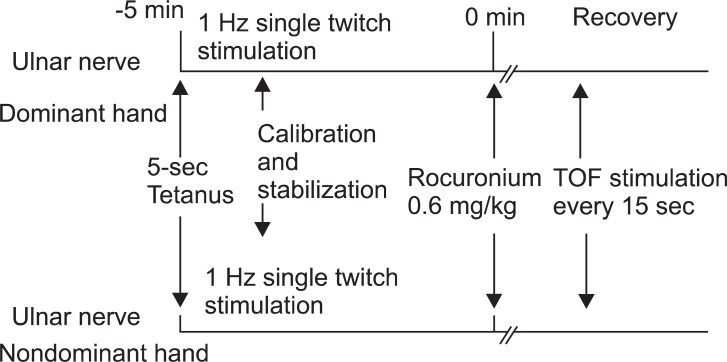
After the loss of eyelash reflex was confirmed, neuromuscular monitoring began immediately. A 5-s 50-Hz tetanic stimulus was applied over both ulnar nerves, respectively. The fingers of both arms were tightly fixed to the armboard, respectively. The calibration and supramaximal stimulation were achieved by the built-in calibration function (CAL 2) of the TOF-Watch SX®, respectively [7]. Stable baseline was completed in at least 2 min (< 5% variation in the first twitch and TOF). After stabilization of control responses, rocuronium (0.6 mg/kg) was administered and tracheal intubation was performed at the disappearance of the TOF response. TOF stimulation (0.2 ms duration, frequency 2 Hz, 2 s duration with supramaximal current) was repeated every 15 s and applied throughout maintenance of anesthesia (Fig. 1). Ventilation was adjusted to maintain end-tidal carbon dioxide between 30 and 35 mmHg. All neuromuscular data were collected on a computer and monitored throughout the study. Skin temperature on the wrist was maintained to more than 32℃ using a wrapping cotton wool and central temperature was maintained to more than 35℃ using a forced air warmer. The time to the onset, maximum effect, and offset of rocuronium were measured. Signal recordings were continued until the TOF ratio to 0.9. Additional doses of rocuronium were given if required. At the end of surgery, the patients received neostigmine (50 µg/kg) and glycopyrrolate (10 µg/kg) if necessary.
Statistical analysis was performed using the SPSS (SPSS for Windows Release 14.0) statistical software package. The sample size (n = 28) was determined based on the following criteria: a significance level of 5% and a power of 80% with an estimated difference of 1 minute at a standard deviation of 0.25 minutes to reach a TOF ratio of 25% between both hands. In the experiment, 31 patients were decided with given 10% wastage rates. Differences in pharmacodynamic variables between TOF ratios on both hands were analyzed using paired Student's t-tests. Linear correlations between the measured parameters were analyzed using the method of least squares analysis. To compare dominant and nondominant hand, the values from each stimulation site were compared by using a Bland and Altman analysis [8]. A P value < 0.05 was considered as statistically significant.
Results
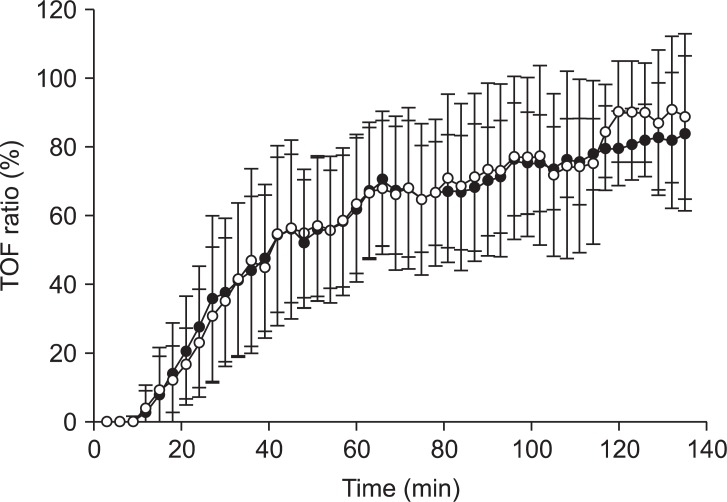
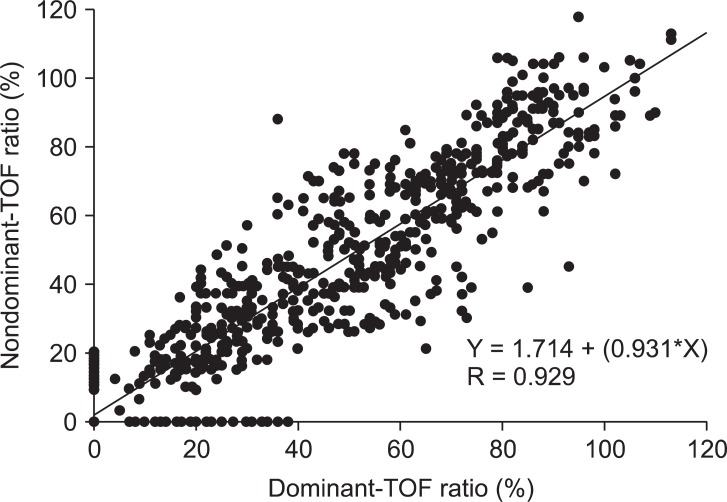
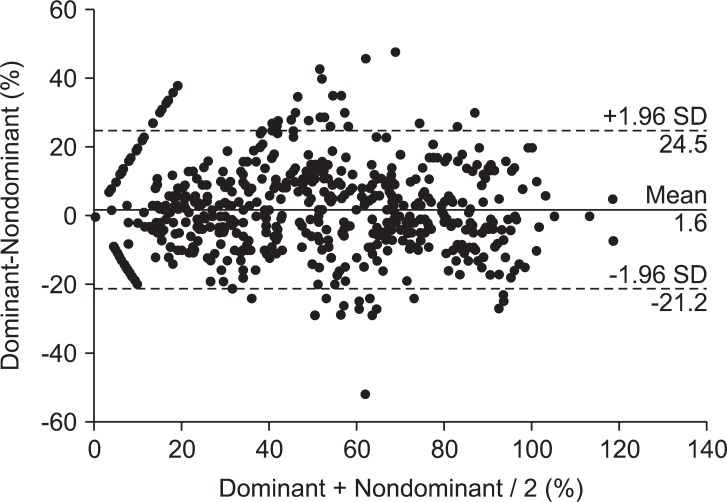
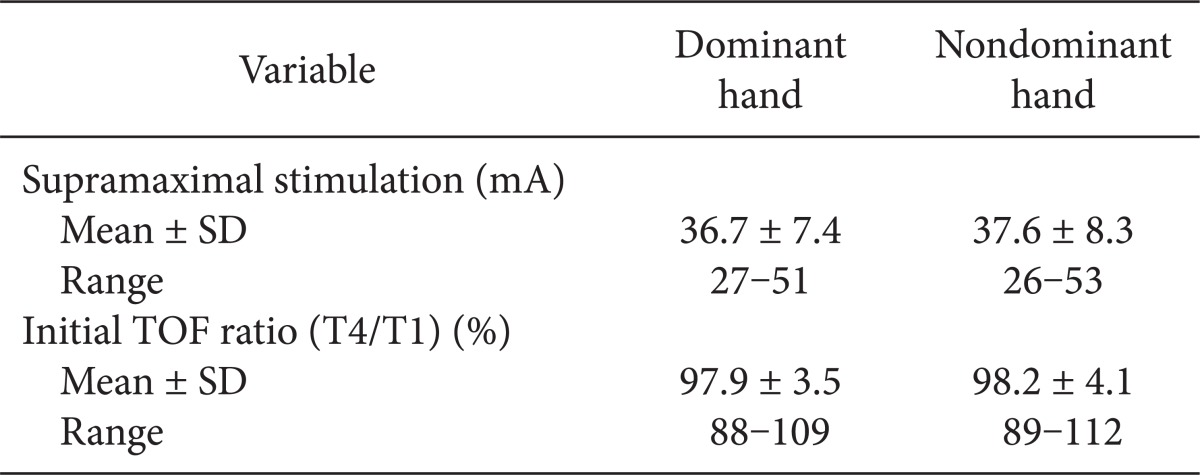
A total of 31 patients were included in the study: 19 men and 12 women (age, 42.9 ± 11.3 years; weight, 71.1 ± 12.3 kg; height, 168.1 ± 10.2 cm; duration of anesthesia, 169 ± 67 minutes). There were 27 right-handed patients and 4 left-handed patients analyzed. There were no differences in the mean supramaximal threshold or mean initial TOF ratio between the dominant or nondominant hands, as presented in Table 1. During recovery, 716 paired TOF ratios were recorded from both hands simultaneously. No statistical differences in the TOF ratios were found during recovery in the dominant and nondominant hands of the same patient (Fig. 2). A regression line of data from the dominant and nondominant hands had an intercept (ic) of 1.714, regression coefficient (b) of 0.931, and correlation coefficient (R) of 0.929 (Fig. 3). There was a bias of 1.6% and the 95% limits of agreement between dominant versus nondominant hands were from -21.2 to 24.5% of the values using a Bland-Altman analysis (Fig. 4).
Discussion
We found pharmacodynamic values of the dominant hand to be comparable to those obtained at the nondominant hand with minimal bias, good correlation, and no statistical differences. The neuromuscular blockade was not influenced by hand dominance.
Motor unit recruitment and firing behavior of the first dorsal interosseous muscle of dominant and nondominant hands in volunteers were compared. The presence of lower average firing rates, lower recruitment thresholds, and greater firing rate/force delay in the dominant muscles suggests an increased percentage of slow twitch fibers from electromyographic studies. These adaptations could potentially lead to a different response to neuromuscular blockade [3]. A different sensitivity between the dominant and nondominant hands was suggested by the potency ratio of vecuronium or 3-desacetylvecuronium at the adductor pollicis muscle via mechanomyography [4]. In another study using phonomyography at the adductor pollicis muscle, Michaud et al. contradicted those results showing no difference in onset time, maximum effect, time to reach 25, 50, 75, and 90% of control twitch response, and TOF ratio of 0.5, 0.7, 0.8, and 0.9 when comparing dominant and non-dominant hands [5]. Nelson et al. [9] examined specific electrical characteristics of voluntary single motor unit action potentials (amplitude, duration, phase change, and rate of rise) from the abductor pollicis brevis and the abductor digiti minimi of the hand. They found no significant differences between muscles in the dominant and non-dominant hands. Despite morphological changes of the muscle in the dominant hand, we did not find any statistical differences between the adductor pollicis muscles of either hand using acceleromyography. The individual differences were wide when using acceleromyography or mechanomyography, although there was no significant mean bias in any recovery parameter between the arms [10]. We also found in Fig. 3 and 4.
Acoustic monitoring of neuromuscular activity at the adductor pollicis muscle during anesthesia correlated closely with monitoring by electromyography, accelorography, and mechanomyography [11]. Phonomyography is a relatively new method for recording neuromuscular blockade at most superficial muscles [6], however, slight movements of the microphone could lead to a significant bias and no commercial devices are currently available. Additionally, phonomyography displayed a slower onset and a faster recovery than mechanomyography at the adductor pollicis muscle after a bolus injection of rocuronium, which was not interchangeable at submaximal levels of neuromuscular blockade [12]. But acceleromyography and mechanomyography can be used interchangeably, when both methods are normalized [13]. For these reasons, we chose to use acceleromyography as a measurement of neuromuscular blockade at the adductor pollicis muscle.
One limitation is that repeated TOF stimulation (every 15 s) during the anesthesia is not exactly same time between the dominant and non-dominant hands due to the calibration mode and fixed fingers to the armboard, respectively.
In conclusion, our results suggest that the dominant or nondominant hand may be used for neuromuscular junction blockade monitoring at the adductor pollicis muscle.
 XML Download
XML Download