

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Pheochromocytoma is characterized by a combination of various clinical manifestations that include the classic triad of severe headache, palpitations and diaphoresis. In addition, hyperglycemia can be caused by overproduction of catecholamines, which are secreted by a catecholamine-secreting neoplasm of adrenal or extra-adrenal chromaffin tissue. We encountered a case of diabetes with an occult malignant adrenal pheochromocytoma, who did not have any classic manifestations. A 37-year-old male was admitted because of polydipsia, polyuria, and weight loss. Fasting blood glucose level was 497 mg/dL, hemoglobin A1c level was 15%, and diabetic retinopathy and peripheral polyneuropathy were also accompanied. Incidentally, right adrenal mass was detected by ultrasonography of abdomen. Urinary excretion of total metanephrine and epinephrine were elevated. Adrenal CT showed a 7.1 cm sized right adrenal cystic mass with enhancing solid portion and hemorrhagic content. The scan with 123I-MIBG revealed the cystic mass with increased rim uptake in the region of right adrenal gland. After removal of the tumor, the increased levels of catecholamine were normalized. Moreover, blood glucose level was normalized without administration of insulin or oral hypoglycemic agents. The pathologic examination showed that the neoplasm was a malignant adrenal pheochromocytoma. We report this case that diabetes was cured after removal of malignant tumor with literature review at first in Korea.
Figures and Tables

Fig. 2
Abdominal CT shows 71 × 63 mm sized cystic mass with enhancing solid portion and hemorrhagic content in right adrenal area.
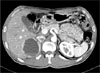
Fig. 3
123I-MIBG scan shows a cystic mass with increased rim uptake, especially posterolateral portion in the right adrenal area.

Fig. 4
Gross findings show an ovoid, pale pink to red and cystic mass from right adrenal gland, measuring 70 × 75 × 68 mm in size and weighing 162.0 gm. There is a remaining adrenal gland tissue on the surface of the cystic mass. On opening the specimen, dark bloody fluid was expelled. The cystic wall of the specimen shows edematous change and thickened. Thickness of the cystic wall measures 1.3 cm in the maximum thickness. There are several pale tan, nodular mural nodules on the inner cystic wall.
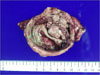
Fig. 5
A. Microscopic findings show atypical tumor cells nests forming vague zellballen area (H&E stain, ×100). B. Tumor cell have profound nuclear pleomorphism with giant cells formation and there are scattered atypical mitotic figures with prominent nucleoli in tumor cells (H&E stain, ×400). C. Tumor cells are focally infiltrative growth pattern into the surrounding capsule, but there is no definite evidence of lympho-vascular invasion in the tumor mass (H&E stain, ×40).

References
1. Bravo EL. Pheochromocytoma: New concepts and future trends. Kidney Int. 1991. 40:544–556.
2. Reisch N, Peczkowska M, Januszewicz A, Neumann HP. Pheochromocytoma: presentation, diagnosis and treatment. J Hypertens. 2006. 24:2331–2339.
4. La Batide-Alanore A, Chatellier G, Plouin PF. Diabetes as a marker of pheochromocytoma in hypertensive patients. J Hypertens. 2003. 21:1703–1707.
8. Yamashita S, Dohi Y, Kinoshita M, Kojima M, Mivagawa K, Sato K. Occult extraadrenal pheochromocytoma treated as diabetes mellitus. Am J Med Sci. 1997. 314:276–278.
9. Saito T, Satoh S, Kawasaki S, Mukasa K, Itoh S, Yamakawa T, Sekihara H. Three patients with adrenal tumors having been treated simply for diabetes mellitus. Biomed Pharmacother. 2000. 54:Suppl 1. 198s–202s.
10. Rizza RA, Cryer PE, Haymond MW, Gerich JE. Adrenergic mechanisms of catecholamine action on glucose homeostasis in man. Metabolism. 1980. 29:1155–1163.
11. Turnbull DM, Johnston DG, Alberti KG, Hall R. Hormonal and metabolic studies in a patient with a pheochromocytoma. J Clin Endocrinol Metab. 1980. 51:930–933.
12. Saccà L, Morrone G, Cicala M, Corso G, Ungaro B. Influence of epinephrine, norepinephrine, and isoproterenol on glucose homeostasis in normal man. J Clin Endocrinol Metab. 1980. 50:680–684.
14. Wiesner TD, Bluher M, Windgassen M, Paschke R. Improvement of insulin sensitivity after adrenalectomy in patients with pheochromocytoma. J Clin Endocrinol Metab. 2003. 88:3632–3636.
15. Emmer M, Gorden P, Roth J. Diabetes in association with other endocrine disorders. Symposium on diabetes. Med Clin North Am. 1971. 55:1057–1064.
16. Stenström G, Sjöström L, Smith U. Diabetes mellitus in phaeochromocytoma. Fasting blood glucose levels before and after surgery in 60 patients with phaeochromocytoma. Acta Endocrinol (Copenh). 1984. 106:511–515.
17. Spergel G, Bleicher SJ, Ertel NH. Carbohydrate and fat metabolism in patients with pheochromocytoma. N Engl J Med. 1968. 278:803–809.
 XML Download
XML Download