

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A 66-year-old woman was resuscitated from a cardiac arrest after completing 1 cycle of cardiopulmonary resuscitation (Supplementary Figure 1). Echocardiography showed severe global akinesia and small pericardial effusion. Coronary angiography was normal. Endomyocardial biopsy was performed. Myocardial pathology confirmed her diagnosis of giant cell myocarditis (GCM) (Figure 1). As a treatment for GCM, she received anti-thymocyte globulin (ATG) followed by cyclosporin A and everolimus (Supplementary Figure 2).1) Follow-up pathological examination showed resolving myocarditis on the 12th hospital day (Figure 2) at 5 weeks after starting treatment. Histological confirmation is essential for verifying GCM in myocarditis.2) Observations in experimental GCM on Lewis rate model suggest that autoimmune mechanisms medicated by CD4+ T lymphocytes are responsible for the pathogenesis of GCM.3) In acute phase, T helper cell type 1 (Th1) is dominant, which may lead to inflammation at the induction of myocarditis. ATG therapy induces a profound decrease in Th1 cell counts.4) Early ATG administered seems to play a key role in alleviating the fulminant inflammation of the heart and resulted in a better clinical course.
You-Jung Choi, MD , Hyun-Jai Cho, MD, PhD
, Hyun-Jai Cho, MD, PhD
, Hyun-Jai Cho, MD, PhD
References
1. Fluschnik N, Escher F, Blankenberg S, Westermann D. Fatal recurrence of fulminant giant cell myocarditis and recovery after initialisation of an alternative immunosuppressive regime. BMJ Case Rep. 2014; 2014:bcr2014206386.
2. Vaideeswar P, Cooper LT. Giant cell myocarditis: clinical and pathological features in an Indian population. Cardiovasc Pathol. 2013; 22:70–74. PMID: 22863545.
3. Kodama M, Matsumoto Y, Fujiwara M, Masani F, Izumi T, Shibata A. A novel experimental model of giant cell myocarditis induced in rats by immunization with cardiac myosin fraction. Clin Immunol Immunopathol. 1990; 57:250–262. PMID: 2208806.
4. Weimer R, Staak A, Süsal C, et al. ATG induction therapy: long-term effects on Th1 but not on Th2 responses. Transpl Int. 2005; 18:226–236. PMID: 15691277.
SUPPLEMENTARY MATERIALS
Supplementary Figure 1
The electrocardiogram (A) and chest x-ray (B) on the first day to the hospital. (A) Sinus rhythm with the low voltage of QRS complexes in the precordial and limb leads. There are no significant ST-segment changes. (B) The chest radiograph shows cardiomegaly with bilateral diffuse infiltrates which suggest cardiogenic pulmonary edema.
Figure 1
Histological findings on endomyocardial biopsy. (A) Diffuse geographic myocarditis with severe necrotic change and inflammatory infiltrate (H&E, ×100). (B) Numerous multinucleated giant cells in nongranulomatous background. (C) Collection of inflammatory cells including variable numbers of giant cells (arrows), histiocyte, T-lymphocyte, and eosinophils. (D) The area with necrotic change and severe inflammation showed negative of desmin. (E) Histiocyte infiltration in myocardium (CD68 staining). (F) T-lymphocyte infiltrate in myocardium (CD3, Pan-T cell marker staining).
H&E = hematoxylin and eosin.
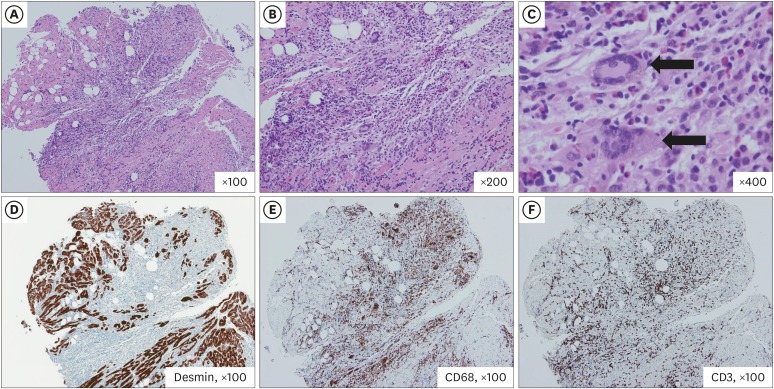
Figure 2
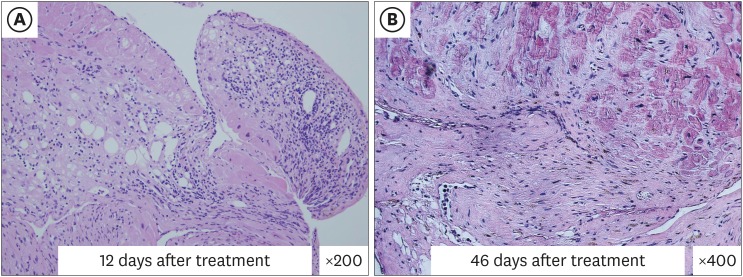
Follow-up endomyocardial biopsy. (A) On 12th day from starting immunosuppressive therapy, myocardial biopsy revealed a marked reduction of the inflammatory infiltrate and the absence of giant cells. The fibrotic and fatty change are seen in the area, where there was necrotic change before treatment (H&E, ×200). (B) On 46th day, massive granulation tissue and fatty change without active myocardial damage was observed (H&E, ×400).
H&E = hematoxylin and eosin.
 XML Download
XML Download