

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Peripheral artery disease (PAD) is generally a manifestation of advanced systemic atherosclerosis. Risk factors strongly associated with the development of PAD include older age, diabetes mellitus (DM), smoking, and male sex.1)2)3) Patients with PAD often have coexisting coronary artery disease (CAD) or cerebral artery disease.4) In general, the presence of PAD is associated with poor prognosis as well as relatively high mortality and morbidity rates.5)
Patients with PAD in the lower extremity may be asymptomatic or may present with symptoms ranging from intermittent claudication, to rest pain, non-healing sores and even gangrene. For moderate to severe symptoms, endovascular or surgical revascularization of diseased arteries is indicated.1)2)3) Endovascular treatment has been traditionally recommended for shorter-duration, limited lesions, whereas surgical options have been chosen for extensive and more complex lesions. However, with the development of newer devices and techniques for endovascular therapy, more complex lesions are increasingly being treated with endovascular options due to their advantages over surgical treatments, including less invasiveness, fewer complications, earlier recovery and shorter hospitalization.
A recent study using Korean Health Insurance data reported the frequency of endovascular treatment in the lower extremity increased more than two-fold from 2004 to 2013, whereas open surgery decreased by 39% over the same period.6) However, knowledge regarding current practice patterns and outcomes of endovascular therapy in Korea is limited. In the present study, baseline clinical and lesion characteristics of Korean patients with lower extremity artery disease who were treated with endovascular methods were investigated.
Subjects and Methods
Study population
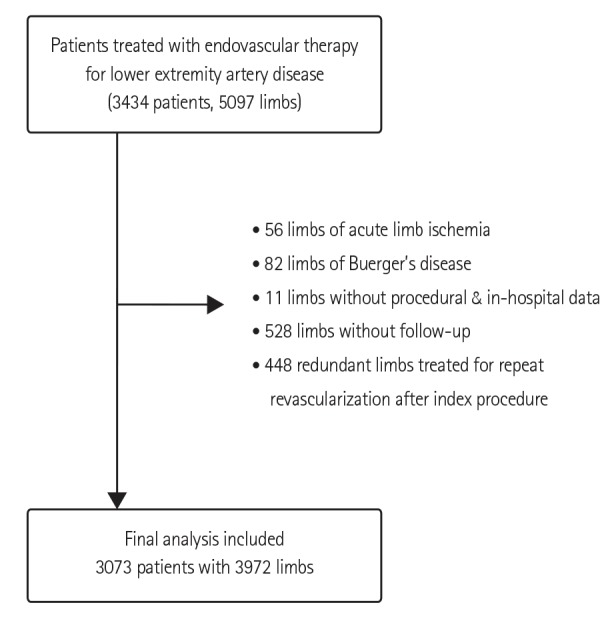
The Korean Vascular Intervention Society Endovascular Therapy in Lower Limb Artery Diseases Registry (K-VIS ELLA) is a multicenter observational study with a retrospective and a prospective cohort of patients with lower extremity artery disease treated with endovascular therapy (ClinicalTrials.gov NCT02748226). The current study encompassed the retrospective patient cohort, which consisted of the datasets of 3434 patients with 5097 limbs treated between January 2006 and July 2015 in 31 Korean hospitals. Inclusion criteria were patients 20 years of age or older and lower extremity artery disease treated with endovascular therapy. A total of 3073 patients with 3972 target limbs from the retrospective cohort were included in the final analysis after exclusion of 56 limbs with acute limb ischemia, 82 limbs with Buerger's disease, 11 limbs without procedural and in-hospital data, 528 limbs without follow-up data after hospital discharge, and 448 limbs treated for repeat revascularization after index procedure (Fig. 1). Data regarding the patient baseline clinical and lesion characteristics as well as medications at hospital discharge were collected from electronic medical records. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the participating hospitals. The institutional review boards of the participating hospitals waived the need for informed consent for this retrospective study.
Definitions
PAD of the lower extremity was defined as the narrowing of a lower extremity artery ≥50%. Claudication was defined as Rutherford category 1, 2, or 3 disease (mild, moderate, or severe claudication, respectively) and critical limb ischemia (CLI) was defined as Rutherford category 4, 5, or 6 disease (ischemic rest pain, minor tissue loss, or major tissue loss, respectively).7) The presence of hypercholesterolemia was defined as total cholesterol level >200 mg/dL or treatment with a lipid-lowering agent prior to hospital admission, as documented in the medical record. Patients were considered current smokers if they smoked at least one cigarette per day. Patients were considered ex-smokers if they had stopped smoking at least 1 month prior to inclusion in the study. Congestive heart failure was defined as the presence of a left ventricular ejection fraction <40%. Anemia was defined according to the criteria of the World Health Organization (<12.0 g/dL in women and <13.0 g/dL in men).8) Chronic kidney disease (CKD) was considered present if the estimated glomerular filtration rate according to the Modification of Diet in Renal Disease Study equation was <60 mL/min/1.73 m2.
Target lesions of the aortoiliac and femoropopliteal arteries were classified according to the TransAtlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II).1) Multilevel disease was defined as the presence of significant obstructive lesions at more than one level in the same limb (aortoiliac, femoropopliteal, and infrapopliteal arteries). Target vessels were classified as aortoiliac, femoropopliteal, anterior tibial, posterior tibial, and peroneal arteries. Prescribed antiplatelet drugs included aspirin, clopidogrel, ticlopidine, ticagrelor, prasugrel, cilostazol, sarpogrelate, triflusal, beraprost, and limaprost. P2Y12 adenosine diphosphate receptor inhibitors included clopidogrel, ticlopidine, ticagrelor, and prasugrel.
Statistical analysis
Continuous variables were expressed as mean±standard deviation and compared with the Student's t-test when normally distributed. Categorical variables were reported as numbers and percentages and compared with the χ2 test or Fisher's exact test. A p value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS (version 23.0; IBM Corp., Armonk, NY, USA).
Results
Clinical characteristics
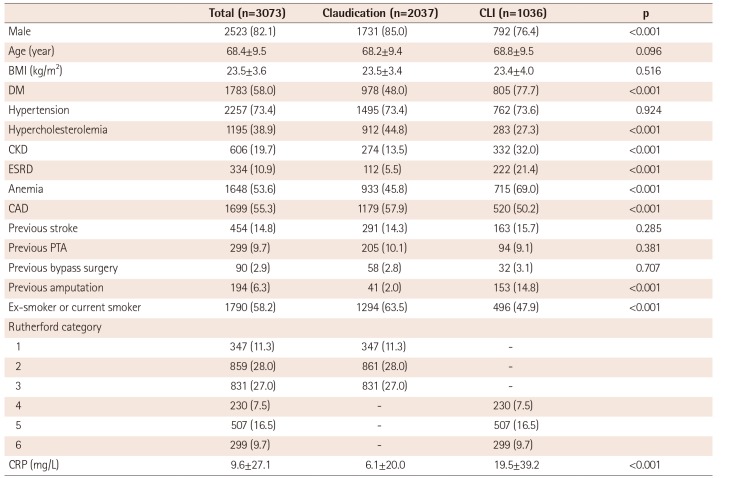
Baseline clinical characteristics of the patients are presented in Table 1. The mean age was 68.3±9.4 years. The majority of patients were males (82.1%) with comorbidities, such as DM (58.0%), hypertension (73.4%), and CAD (55.3%). More patients presented with intermittent claudication (n=2039, 66.3%) than with CLI (n=1036, 33.7%). Compared with CLI patients, subjects with claudication were more frequently male and smokers (current or ex-smokers) and more likely to have hypercholesterolemia and coexisting CAD. However, DM, CKD, end-stage renal disease (ESRD) requiring dialysis, anemia, and a history of amputation were more frequently observed in patients with CLI than in subjects with claudication. C-reactive protein was significantly higher in patients with CLI than in subjects with claudication (19.5±39.2 vs. 6.1±20.0 mg/L, p<0.001).
Lesion characteristics
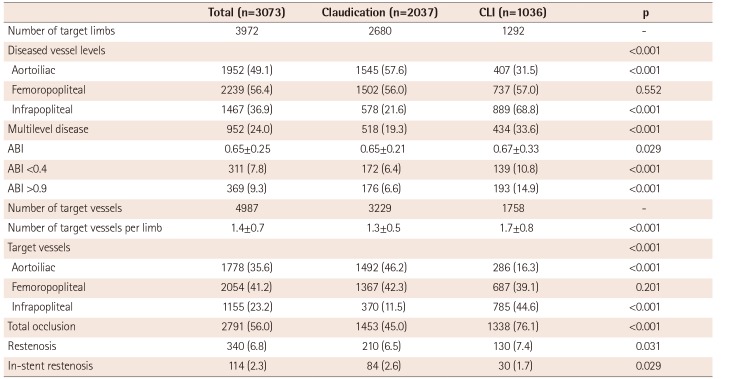
A total of 4987 target vessels in 3972 limbs were treated with endovascular therapy (Table 2). Patients with claudication had 3229 target vessels in 2680 limbs and patients with CLI had 1758 target vessels in 1292 limbs. The mean number of treated vessels per limb was higher in patients with CLI than in subjects with claudication (1.7±0.8 vs. 1.3±0.5, p<0.001).
Overall, the femoropopliteal artery (56.4%) was the most commonly affected vessel, followed by the aortoiliac (49.1%) and infrapopliteal arteries (36.9%). The frequency of femoropopliteal artery involvement was similar between the claudication and CLI groups. However, the aortoiliac artery was more frequently involved in the claudication group (57.6% vs. 31.5%, p<0.001), whereas the infrapopliteal artery was more frequently affected in the CLI group (68.8% vs. 21.6%, p<0.001). Multilevel disease was more frequently found in the CLI group than in the claudication group (33.6% vs. 19.3%, p<0.001). However, the ankle-brachial index (ABI) was higher in the CLI group than in the claudication group (0.65±0.21 vs. 0.67±0.33, p=0.029). However, the CLI group included more patients with an ABI <0.4 and >0.9 than the claudication group.
In the entire study population, the femoropopliteal artery (41.2%) was the most common target vessel for endovascular treatment, followed by the aortoiliac (35.6%) and infrapopliteal arteries (23.2%). The aortoiliac arteries were the most common target vessels in the claudication group, whereas the infrapopliteal arteries were the most common target vessels in the CLI group. Total occlusions and restenosis lesions, including in-stent restenosis lesions, were more frequent in the CLI group than in the claudication group.
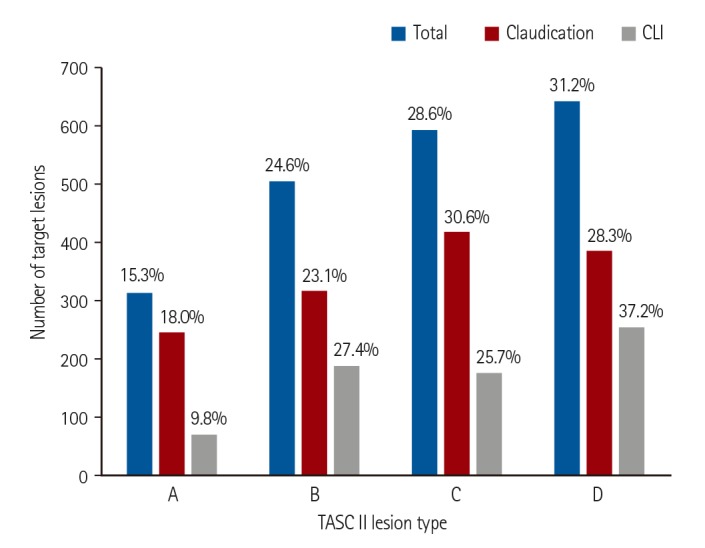
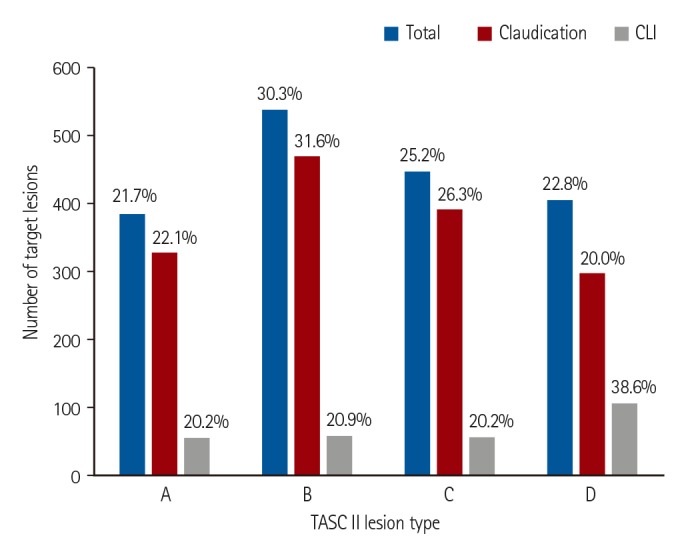
Among the aortoiliac lesions, TASC II classification type B was the most frequent lesion, followed by types C, D, and A lesions, in descending order of frequency (Fig. 2). The distribution of lesion types was significantly different between the claudication and CLI groups (p<0.001). Whereas type B was the most common lesion type in the claudication group, type D was the most frequently treated lesion type in the CLI group. Among the femoropopliteal lesions, type D lesions were the most frequent lesions, followed by types C, B, and A, in descending order (Fig. 3). The distribution of femoropopliteal lesion types was also significantly different between the claudication and CLI groups (p<0.001). Whereas type C was the most common lesion type in the claudication group, type D was the most frequently treated lesion type in the CLI group.
Medications
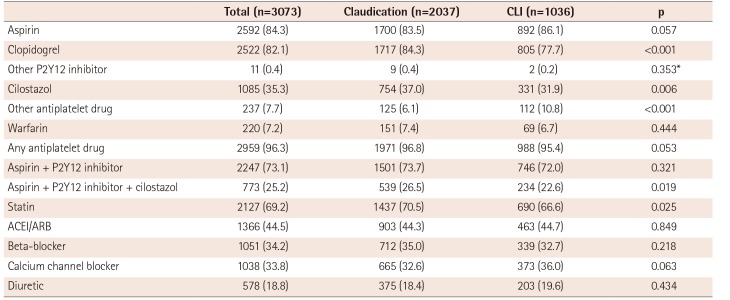
The medications at hospital discharge are summarized in Table 3. Overall, prescription rates of antiplatelet drugs were relatively high in both the claudication and CLI groups. The claudication group showed a trend of more frequent antiplatelet drug use than the CLI group, although the difference did not reach statistical significance (96.8% vs. 95.4%, p=0.053). Compared with the CLI group, the claudication group exhibited more frequent use of clopidogrel (84.3% vs. 77.7%, p<0.001), cilostazol (37.0% vs. 31.9%, p=0.006), and triple antiplatelet therapy including aspirin, P2Y12 inhibitor, and cilostazol (26.5% vs. 22.6%, p=0.019). Combination therapy with aspirin and a P2Y12 inhibitor was used in 73.1% of patients, but showed no difference between the claudication and CLI groups (73.7% vs. 72.0%, p=0.321). Statins were prescribed in only 69.2% of patients. The claudication group received statins more frequently than the CLI group (70.5% vs. 66.6%, p=0.025). The use of antihypertensive drugs was not significantly different between groups.
Discussion
The prevalence of lower extremity artery disease in Korea remains unknown; however, with progressive aging of the Korean population, the number of patients with PAD undergoing endovascular or surgical treatment is rapidly increasing. According to a recent study based on National Health Insurance data, the total number of procedures increased each year from 2008 to 2012 by 20 to 25%.9) Among the total procedures performed for treatment of lower extremity artery diseases, 80 to 95% are endovascular treatments. Furthermore, the number of endovascular treatment centers increased from 120 in 2008 to 163 in 2012. However, to date, minimal representative data exist regarding the characteristics and outcomes of patients undergoing endovascular treatment for lower extremity artery disease in Korea. Thus, we established a Korean multicenter registry containing a retrospective and prospective cohort to address this issue. The present study is the first report on the baseline characteristics of the retrospective cohort.
Male sex, older age, DM, smoking, hypertension, and hypercholesterolemia are established risk factors for atherosclerosis and PAD.1)2)3) In our study cohort, the mean age was 68 years, and the majority of patients were male (82.1%) and current smokers (58.2%) with DM (58.0%) and hypertension (73.4%). Atherosclerotic diseases, such as CAD (55.3%), stroke (14.8%), and CKD (19.7%), frequently coexisted with PAD in our patients. Approximately two-thirds of patients presented with intermittent claudication and one-third with CLI. In previous studies, chronic heavy smoking, older age, DM, and CKD were identified as risk factors for CLI.1)10)11) Similarly, we found DM and CKD, including ESRD, were more common in the CLI group than in the claudication group. However, no significant difference in age was observed between the claudication and CLI groups. Male sex, hypercholesterolemia, and smoking were less frequent in the CLI group than the claudication group. Thus, in our patient cohort, DM and CKD were the most important factors in the development of CLI. In particular, DM was present in 77% of the CLI patients. This prevalence of DM in CLI patients is similar to that reported in Japanese patients with CLI (68 to 71%)12)13) but higher than the prevalence in European or American patients with CLI (44.1 to 61%).14)15)16)17) Conversely, the prevalence of CKD (32%) among CLI patients in our study was lower than in the Japanese (61%)12) or European study cohorts (57%) of patients with CLI.15)
The basic pathophysiology of CLI involves macro- and microvascular defects that lead to reduced arterial perfusion insufficient to meet the resting tissue demands for oxygen and nutrients. Endothelial damage caused by inflammation and oxygen radicals, inappropriate platelet aggregation, tissue edema, and inadequate angiogenesis are hypothesized to contribute to the development of CLI.11) DM and CKD are two representative diseases with increased level of systemic inflammation and an excessive burden of oxygen radicals. Patients with DM and renal dysfunction typically have diffuse, severe infrapopliteal arterial occlusive disease. Patients with CKD, and especially those with ESRD, are prone to developing medial calcifications, which are commonly observed in the tibial and femoral arteries. Severe vascular calcifications are the major obstacles to endovascular treatment.
In the present study, the femoropopliteal artery was the most common target of endovascular treatment for the entire study cohort. However, the aortoiliac arteries were the most common target vessels in the claudication group, whereas infrapopliteal arteries were most commonly treated in the CLI group. Complex lesions, such as TASC II type D lesions, were frequently treated with endovascular therapy. Among the femoropopliteal artery lesions, type D lesions were the most common targets (31.2%). Among the aortoiliac lesions, 22.8% were type D lesions. International guidelines primarily recommend surgery as the treatment of choice for type D aortoiliac or femoropopliteal lesions.1)2)3) European guidelines suggest that type D lesions can be treated by endovascular procedures in patients with severe comorbidities if they are performed by an experienced team.2) There may be several reasons for the preferential use of endovascular therapy for type D lesions observed in our cohort. First, patient factors may have played a role. Patients requiring treatment were frequently old and had comorbidities such as CAD, previous stroke, and CKD. Often, patients preferred to undergo less invasive procedures. Second, physician factors may have also played a role. This is a retrospective cohort of patients treated by interventional cardiologists. Therefore, physicians tended to treat complex lesions primarily with endovascular techniques.
In general, there were relatively high prescription rates for antiplatelet drugs after endovascular therapy in both the claudication and CLI groups. Nevertheless, only 73.1% of patients received combination antiplatelet therapy consisting of aspirin plus a P2Y12 inhibitor and only 69.2% of patients received a statin. Dual antiplatelet therapy with aspirin and a thienopyridine is generally recommended for at least 1 month after endovascular therapy, especially when performed with stent implantation.2)3) In the present study, the rate of antiplatelet therapy using at least 1 antiplatelet drug was high (96.3%); however, the 73.1% rate of dual antiplatelet therapy with aspirin plus a P2Y12 inhibitor at hospital discharge was lower than expected. In patients with PAD, guidelines recommend lipid-lowering therapy with a low-density lipoprotein (LDL) cholesterol goal of <70 mg/dL and/or a ≤50% reduction in LDL cholesterol.2)3) Previous studies demonstrated benefits of statins in reducing mortality and cardiovascular events in patients with PAD.18)19)20) Thus, the statin prescription rate of approximately 70% at hospital discharge was disappointing. The statin prescription rate was even lower (66.6%) in patients with CLI. Therefore, approximately 30% of patients in our cohort did not receive optimal post-procedural medical treatment to prevent adverse cardiovascular events. There may have been various reasons for not prescribing adequate antiplatelet agents or statins. However, the reasons could not be clarified within the limits of this retrospective study. This rate of non-adherence to guidelines for optimal medical treatment is high and alarming. Physicians' awareness of this issue should be increased as well as the effort in providing optimal treatment to prevent adverse cardiovascular events.
This study had several limitations. First, due to the retrospective study design, inherent limitations existed. Second, endovascular treatment was performed in this registry study by interventional cardiologists. Therefore, the study may not represent patient characteristics or practice patterns of endovascular practitioners of other specialties, such as interventional radiologists or vascular surgeons. Third, the lesion characteristics were not analyzed in a central imaging core laboratory.
In conclusion, the majority of Korean patients with PAD exhibited conventional risk factors, such as male sex, older age, DM, and hypertension with coexisting CAD. Complex lesions were frequently treated with endovascular therapy. However, the rate of adherence to guidelines regarding post-procedural medical treatment should be improved in the future.
 XML Download
XML Download