

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Left ventricular hypertrophy (LVH) is associated with an increased risk of cardiovascular events.1) Electrocardiography (ECG) and echocardiography (Echo) are generally used to diagnose LVH. Although Echo is preferred because of its higher sensitivity, ECG is widely used in large-scale research studies and in clinical practice to detect LVH due to its convenience and cost-effectiveness (although it generally has low sensitivity). Additionally, ECG-LVH and Echo-LVH predict mortality independently and provide different prognostic information.2) Several ECG criteria are available to assess LVH.3) Among them, gender-neutral Sokolow-Lyon voltage (Sok V) and gender-specific Cornell voltage criteria are commonly used as voltage criteria. Molloy et al.4) suggested that the simple product of voltage and QRS duration is useful to identify LVH more accurately than voltage criteria alone.
Some studies have shown superiority of the Cornell-based criteria {Cornell voltage and Cornell product (Cor P)} to the classic Sok V criteria and the Romhlit-Estes score for identifying LVH.5)6) The Cornell-based criteria were used to diagnose LVH in the Losartan Intervention For Endpoint (LIFE) study because of their usefulness.7)8) However, most studies have been conducted on Caucasians, and the diagnostic performance of Cornell-based criteria for the Korean population is unknown. Although the 2007 European Society of Hypertension-European Society of Cardiology Guidelines adopted both the Cor P and Sokolow-Lyon criteria as ECG criteria for LVH,9) they have different diagnostic performances among races.10)
The aim of this study was to compare the diagnostic performance of the Cornell criteria and that of the Sokolow-Lyon criteria and to define their race-specific cut-off values in the Korean population.
Subjects and Methods
Study population
In a retrospective cross-sectional design, data from consecutive patients visiting the Cardiology Center at Hanyang University Hospital, Seoul, Korea from September 2005 to April 2006 were analyzed. A total of 1120 patients who underwent ECG and Echo were enrolled. Exclusion criteria were cases with incomplete clinical or hemodynamic data and patients with myocardial infarction, valvular heart disease (i.e., grade II or more valvular regurgitation or any valvular stenosis), LV dysfunction, pericardial disease, chronic obstructive pulmonary disease, bundle branch blocks, and atrial fibrillation or flutter based on a clinical history and examination. After applying the exclusion criteria, 332 patients remained.
Electrocardiographic measurement
A standard 12-lead ECG was recorded at 25 mm/sec paper speed and 1 mV/cm and were interpreted by a single reader at Hanyang University Seoul Hospital who was blinded to the patient's ECG data. He measured QRS duration, R-wave amplitudes in leads aVL, V 5, and V 6 and S-wave amplitudes in leads V 1 and V 3 and calculated four ECG criteria: Sok V,11) Cornell gender-specific voltage (Cor V),12) the Sok P, and the Cor P.4) LVH was conventionally defined as a Sok V amplitude of (SV 1 or V 2+RV 5 or V 6) ≥35 mm, a Cor V of (RaVL+ SV 3) ≥28 mm for men and ≥20 mm for women, and a Cor P of (QRS duration times Cornell voltage combination with 8 mm added in women) ≥2440 mm×ms. There is no recognized cut-off value for Sok P (QRS duration times for the Sok V combination). Therefore, we established a cut-off value of 3340 mm×ms for Sok P to provide the same specificity as the Cor P, similar to a previous study.13)
Echocardiographic measurement
A single sonographer performed all tests with a commercially available machine (iE33; Philips Medical Systems, Andover, MA, USA) using a 1-5 MHz transducer at Hanyang University Seoul Hospital. He had no knowledge of the patient's clinical data. Images were obtained in the supine and left lateral positions using parasternal long-axis and short-axis views and in the apical four and two-chamber views. LV measurements were performed at or just below the mitral valve tips using the leading edge-to-leading-edge method, according to the recommendations of the American Society of Echocardiography (ASE),14) with the M-mode guided by a two-dimensional examination. LV systolic and diastolic diameters as well as interventricular septal and posterior wall thickness were measured at end-diastole, which was defined by the beginning of the QRS complex. Left ventricular mass (LVM) was calculated using the corrected ASE formula by Devereux et al.15)
LVM=1.04×[{LVID+posterior wall thickness (PWT)+interventricular septal thickness (IVST)}3-LVID3]×0.8+0.6
The LVID, PWT, and IVST represented the LV internal dimension (cm), LV posterior wall thickness (cm), and IVST (cm), respectively. Left ventricular mass was indexed for body surface area (LVM/BSA, g/m2), which was calculated by the Dubois formula, and for height2.7 (LVM/height2.7, g/m2.7), as recommended by De Simone et al.16) We set the cut-off value for LVH as LVM/BSA ≥116 g/m2 in males and ≥96 g/m2 in females; LVM/height2.7 ≥49 g/m2.7 in males and ≥45 g/m2.7 in females.17)
Statistical analysis
All measured values are reported as mean±standard deviation for continuous variables and as frequencies and percentages for categorical variables. Student's t-test was used to assess the difference in the means, and categorical variables were analyzed with the chi-square test between genders. Pearson's correlation coefficient was used to determine the degree of correlation between the four ECG criteria and the two indexed LVMs (LVMI).18) Receiver operating characteristic (ROC) curves were used to compare the performance of the four ECG criteria over a range of specificities. Pairwise comparisons of the four ECG criteria were done using differences between the areas under the curves (AUC). We compared the sensitivities and specificities for the four ECG criteria using conventional cut-off values. Additionally, the sensitivities and corresponding cut-off values were extracted for each criterion at fixed specificity levels of 90, 95, and 100%, and we compared them at a fixed specificity level of 95%, which is the most widely used level in the literature.4)6) A two-tailed p<0.05 was considered significant. All analyses were performed using Statistical Package for the Social Sciences (SPSS) version 18.0 (SPSS Inc., Chicago, IL, USA) and Medcalc version 9.1 (Medcalc software, Mariakerke, Belgium).
Results
Demographic characteristics, electrocardiography measurements, and echocardiography values
Mean ages were 51.75±14.12 years for males and 54.63±13.17 years for females (p=0.055) and more males were included than females (11.3% vs. 4%, p=0.013) (Table 1). Mean body mass index (BMI) was not different (25.07±3.36 vs. 24.60±3.77 kg/m2, p=0.237) and the distribution of BMI was similar (p=0.358), but mean BSA was significantly different (1.81±0.15 vs. 1.59±0.12 m2, p<0.001) in males and females, respectively. No significant difference was observed in the prevalence of hypertension, diabetes mellitus, blood pressure, or heart rate between genders. Males had significantly higher mean ECG measurements than those of female for all criteria, including QRS duration, except the Cor P, for which females had significantly higher means (p<0.01). Mean LVM/BSA was higher in males than that in females (115.23±27.83 vs. 101.89±25.08 g/m2, p<0.001), but that of LVM/height2.7 was not different (51.47±14.87 vs. 49.16±14.07 g/m2.7, p=0.147). No difference in the prevalence of LVH by the two LVMI was observed between genders (LVM/BSA; p=0.101, LVM/height2.7; p=0.582).
Correlation between the four electrocardiography criteria and the two type indexed Left ventricular masses
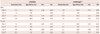
All four ECG criteria were significantly correlated with the two types of LVMI (r values, 0.217-0.507, p<0.01) (Table 2). Cor V and Cor P had a higher correlation coefficient than that of Sok V and Sok P in both genders, but this result was significant only in females. The product of QRS duration and voltage tended to improve the correlation in Sok V, but this result was not significant.
Comparison of the performance of the four electrocardiography criteria using receiver operating characteristic curves and conventional cut-off values
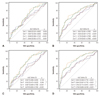
Comparison of the AUC showed that the Cor V and Cor P had higher AUCs than those of Sok V or Sok P in both genders (Fig. 1). Cor V had the highest AUC in both genders (AUC in LVM/BSA: 0.648 in males and 0.735 in females, p<0.001; AUC in LVM/height2.7: 0.687 in males and 0.782 in females, p<0.001).
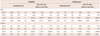
In pairwise comparisons of AUC for each criterion, AUC of the Sok V and that of Cor V were considerably different for LVM/height2.7 but not for LVM/BSA (males: difference between areas=0.042, p=0.484 for LVM/BSA; difference between areas=0.120, p=0.041 for LVM/height2.7, females: difference between areas=0.098, p=0.066 for LVM/BSA; difference between areas=0.138, p=0.007 for LVM/height2.7). However, the difference in AUC between the Sok P and Cor P was significant only in females for LVM/height2.7 (difference between areas=0.080, p=0.050 for LVM/BSA; difference between areas=0.112, p=0.023 in LVM/height2.7). No significant difference was observed between Sok V and Sok P as well as between Cor V and Cor P except in female cases for LVM/height2.7 (difference between areas=0.026, p=0.038 in LVM/height2.7). The sensitivities for the conventional cut-off values were generally low, particularly in males using Cor V and Cor P (1.2-1.4% and 9.3-9.9%, respectively) and in females using Sok V and Sok P (7.1-7.5% and 8.1-8.6%, respectively) (Table 3). The test-negative likelihood ratio ranged from 0.82 to 0.99 due to the low sensitivities of the four LVH criteria.
Comparison of performance of the four electrocardiography criteria using revised cut-off values
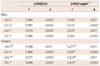
The sensitivities of gender-specific cut-off values for the four ECG criteria at a fixed specificity level of 95% varied considerably, ranging from 9.3 to 30.3% (Table 4). Although Sok P had the highest sensitivity for males (21.1% in LVM/BSA), Cor V generally had better sensitivity (LVM/BSA: 19.7% in males and 22.6% in females; LVM/height2.7: 18.6% in males and 30.3% in females, respectively) than that of the other criteria in both genders.
Discussion
Several Korean studies have investigated the performance of ECG criteria for LVH, and they have been conducted to improve ECG criteria for assessing LVH.18-21) But, the performance of the Cornell-based criteria has never been studied in Korea. Among various ECG criteria, voltage criteria are most convenient and they do not demand a PC-based analysis. Moreover, the Cornell-based criteria have been recently used and recommended in large-scale studies.7-9) Xie and Wang22) used the Cornell-based criteria to assess LVH in Chinese patients with hypertension, and their performance tended to be better than that of other criteria. Rodrigues et al.6) showed that Cor V had a closer association with LVM and better performance in the analysis of AUC of ROC than that of Sok V. as we demonstrated in this study. However, pairwise comparisons were not conducted in those studies. Comparing only the AUC may be insufficient to precisely determine ECG criteria performance. In this study, the difference between each AUC was analyzed to determine whether it was statistically significant and to measure the performance of the ECG criteria.
The main finding of this study was that Cor V performed better than Sok V in the correlation with the two LVMIs, the AUC of the ROC in both genders, and in pairwise comparisons of LVM/height2.7. Another interesting finding was that with revised cut-off values under a fixed specificity of 95%, the Cor V also showed better sensitivity than that of any other criteria.
Noble et al.23) analyzed vector cardiographic changes induced by LVH to explain such better performance of Cor V. The increased LVM orients the electric forces horizontally (corresponding to the RaVL) and posteriorly (corresponding to the SV 3). Furthermore, the V 3 lead is closer to the LV and is probably less influenced by variations in the distance between the myocardium and the leads. Considering this better performance of the Cor V with revised gender-specific cut-off values, we can postulate that gender-specific criteria are still useful in Korean subjects even though reliable cut-off values are not yet available. Revised gender-specific cut-off values are also strongly supported by the finding that Cor V sensitivity at conventional cut-off values was too low to be applied to Koreans. However, further studies are needed to confirm the clinical usefulness of gender-specific cut-off values in Korean subjects.
We observed gender differences in the performance of the ECG criteria. Although Cor V had better performance than that of Sok V in both genders, the sensitivity of Cor V in females was stronger than that in males. Previous studies have shown that gender may influence ECG criteria sensitivity and this could affect the ECG performance for LVH.13)24) Barrios et al.25) suggested that there are pathophysiological differences between genders regarding establishing and developing LVH. In the LIFE study, there were more female patients with ECG-LVH by Cor P than that of males.
In contrast with LVM/BSA, mean LVM/height2.7 in our study was not significantly different between genders, which was consistent with a previous study.26)A better correlation between the Cornell-based criteria and the two types of LVMI, regardless of gender, was also found in a previous study.22) We expect that LVM/height2.7 to be a similar clinical value for Korean subjects. Further study may be needed to determine whether index-specific cut-off values are clinically useful to predict LVH.13)
Revised cut-off values of the Cor V (20 mm in males and 16 mm in females) improved the sensitivity in both genders by up to 30.3%. This tendency was also found in a previous study.27) However, revised Cor V cut-off values in males were lower than those in previous studies,6)12)22)27) and although the mean Cor V values were significantly different in males and females, the differences were not apparent (13.57±5.33 vs. 11.62±5.14 mm, p=0.001). These findings suggest that a gender difference in the cut-off values for Koreans may be smaller than that of conventional cut-off values. But, because conventional Cor V cut-off values were obtained from a sample of young normotensive individuals in whom the magnitude of ECG voltage was significantly different between genders,12)28)29) relatively older subjects in our study may have biased the cut-off values. Theoretically, the compositional changes in myocardial fibrosis, which are potentially complicated by hypertension, may have reduced the correlation between electrical voltage and LVM. Therefore, further study in representative young subjects showing clear differences between genders is needed to set reasonable gender-specific cut-off values.
Some limitations were noteworthy in this study. Because we used data from patients, generalizing our findings may be limited to a patient population in which the prevalence of hypertension and diabetes mellitus is somewhat different from that of the general population. The age distribution may have been different from that of the general population (there were fewer young females than young males). However, test characteristics such as sensitivity and the likelihood ratios are indispensable in situations such as hypertension, diabetes, and the elderly in real world situations. A small number of obese patients also participated in this study, and obesity may affect LVH. Therefore, we used LVM/height2.7 as LVMI besides LVM/BSA, which is obesity-independent. Additionally, as some of the patients were previously on pharmacological treatment, this may have affected the results. Therefore, this study may not be sufficient to generalize to all Koreans. Although the Cor V sensitivities improved with the revised cut-off values, they were not satisfactory because of the low sensitivity of the voltage criteria. The accuracy of ECG criteria for diagnosing LVH is not enough. A scoring system such as the Romhilt-Estes or Perugia scores may improve sensitivity, 30) but they could diminish specificity and may not be useful for a large population. Furthermore, none of the more sophisticated indices is clearly superior to the voltage criteria.19) Therefore, the ECG criteria cannot be considered a "SpPIn" (specific, positive, in) test for the diagnosis of LVH in patients with hypertension20) and the clinician should assess the cost effectiveness of different diagnostic strategies.
In conclusion, the gender-specific Cor V had better overall performance in Korean subjects. Because conventional Cor V cut-off values may not be appropriate for the total Korean population, we suggest revised Cor V cut-off values of 20 mm for males and 16 mm for females. A further examination of the general population may be necessary to acquire more accurate cut-off values.

 XML Download
XML Download