

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The transfemoral approach using the Seldinger technique has been considered the preferred method for both coronary and peripheral arteriography. Local vascular complications of transfemoral arteriography, advocated by Judkins,1) are rare (5% to 10%) but potentially serious.2)3) A Meta analysis found major access complications in 0.3% of cases that used the transfemoral approach (p<0.0001).4) Complications that require surgical correction are more common when the arterial puncture site is outside the common femoral artery. The types of complications associated with the transfemoral approach were variable and included groin hematoma, arteriovenous fistula (AVF), false aneurysms, arterial dissection, arterial perforation and neurological deficits.5) Transradial access for coronary artery intervention dramatically reduces these access site complications.1) Only three cases of AVF have been reported in previously published studies of radial catheter-based procedures (Table 1).6)7) We report here a rare case of AVF, which developed after coronary angiography perfomed using the transradial approach.
Case
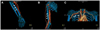
A 67-year-old man visited our hospital with a palpable mass on his right wrist. He had previously been treated for primary hypertension and ischemic heart disease. One year ago he underwent percutaneous coronary intervention (PCI) for unstable angina, along with implantation of a drug-eluting stents in the proximal and distal right coronary artery and in the left anterior descending artery using the transradial approach without complication. Blood pressure was 109/62 mmHg, heart rate was 90 beats/minute, and there were no other abnormal findings after physical examination and biochemical tests. An electrocardiogram showed T-wave inversion in leads II and III, and aVF without interval change. He complained of a palpable mass (3×1.5 cm) on his right wristat the previous puncture site of the radial artery, where palpated thrill, auscultated bruit, and edema were observed. A vascular ultrasound scan revealed suspicious turbulent flow in the systolic and diastolic phase at the previous puncture site of the right radial artery, which suggested AVF or pseudoaneurysm (Fig. 1). Upper extremity computed tomography (CT) angiography revealed AVF between the right radial artery and the adjacent cephalic vein around the right wrist. There was contrast filling in the right cephalic, brachial (Fig. 2A, white arrows), axillary (Fig. 2B, white arrows), and subclavian veins, and the superior vena cava (Fig. 2C, white arrows) in the arterial phase through the fistula between the radial artery and the cephalic vein. The patient was referred to a vascular surgeon and received surgical ligation of the AVF.
Discussion
An AVF is an abnormal connection or passageway between an artery and a vein. It may be congenital, surgically created for hemodialysis treatment, or pathologically acquired via trauma or erosion of an arterial aneurysm. An AVF results in a disruption of the normal blood flow pattern. Normally, oxygenated blood flows to tissues through arteries and capillaries. Following the release of oxygen, the blood returns to the heart in veins. In case of AVF, the blood bypasses the capillaries and tissues, returning directly to the heart. Arterial blood has a higher blood pressure than venous blood, and causes swelling of veins involved in the fistula.
Percutaneous transfemoral arterial cardiac catheterization has reached widespread acceptance and achieved remarkable growth as a tool for diagnostic and therapeutic endovascular intervention. In the large scale prospective study of Kent et al.8) which included 1,838 patients, the incidence of iatrogenic AVF was 0.3%. The majority of patients who suffer from an iatrogenic AVF do not develop clinical signs of hemodynamic significance. All patients were routinely examined by the clinician before and after catheterization, including auscultation of both groins. In cases where there is clinical suspicion of a vascular complication, a duplex scan can be performed. Three different therapeutic strategies have been recommended so far to treat femoral iatrogenic AVF. These are surgical repair, implantation of covered stents, and ultrasound guided compression.9) Among them, Surgical repair has frequently been recommended for patients with iatrogenic AVF.9) The use of transradial access for PCI has increased dramatically since the first report of transradial cardiac catheterization in 198910) and PCI in 1993.11) The transradial approach is associated with fewer vascular access complications than the transfemoral approach.5) Furthermore, an AVF of the radial artery is rare, and even less common than radial artery pseudoaneurysm because only small veins are present in the vicinity of the radial artery. But care must be taken to prevent vascular complications even when we perform coronary procedures using transradial access.
In this case, we report a rare case of radial AVF, which developed after coronary angiography perfomed using a transradial approach. Vascular ultrasound scans and CT angiography can help physicians to evaluate AVF precisely.


 XML Download
XML Download