

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Carney complex(CNC) is a rare disease characterized mainly by myxomas, spotty skin pigmentations, and multiple neuro-endocrine tumors.1)2) CNC appears to be a familial disease,1) transmitted in an autosomal dominant pattern.2) However, sporadic forms of the disease has also been reported.1) Clinical manifestations of CNC may not be fully expressed simultaneously. So CNC may be viewed as a developmental disorder.1) We report a case of CNC, which was in sporadic form, found 11 years after resection of recurrent cardiac myxomas.
Case
A 37-year-old female patient presented with multiple, tender breast masses and intermittent headache. We had previously reported this patient in 1984 as biatrial myxomas and in 1994 as recurrent left atrial and ventricular myxomas(Fig. 1A, B), and at those times, she did not have any other extracardiac myxomas and skin lesions. On her second admission, multiple cerebral aneurysms were noted but aneurysmectomy could not be performed because of patient's refusal. After the second resection of cardiac myxomas, she did not have medical follow up in our hospital. In 1997, a 5 mm-sized extruding mass was developed on her right forearm and the mass was recurred at the same site shortly after the resection in a local hospital. And then in 2003, a 5 mm-sized extruding mass was developed in her right nostril, and from that time, she had suffered from intermittent headache. On the autumn in 2004, discharges from her left nipple and multiple tender masses in her breasts were developed. She was referred for further evaluation of these multiple extruding masses and of the current state of previously resected myxomas.
On admission, her vital signs were unremarkable. On physical examination, she had numerous freckles on her lips and perioral skin(Fig. 2). Bean sized soft masses were observed in her right nostril(Fig. 3A) and on her right forearm(Fig. 3B). Various sized tender masses were palpated in her breast. Transthoracic and transesophageal echocardiography revealed no residual cardiac myxoma. Breast MRI showed multiple high signal mass lesions at T2 weighted images.
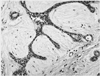
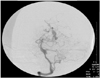
Pathologic examination of breast lesions showed fibroadenomas with abundant myxoid components(Fig. 4) but there was no evidence of malignancy. Both MRI and pathologic findings were compatible with myxomas. Because breast lesions were multiple and numerous, we could not excise them all. Pathologic findings of cutaneous showed spindle and stellate shaped cells which formed vascular mucinous matrices. These were consistent with myxomas. The patient was diagnosed as Carney complex with recurrent cardiac myxomas, cutaneous myxomas, breast myxomatosis and spotty skin pigmentations. And then we tried to look for the evidences of neuro-endocrine tumors. IGF-1 and prolactin were slightly elevated with the values of 573.3 ng/mL(140-400 ng/mL) and 30.21 ng/mL(6-29.9 ng/mL) respectively. So we performed 75 gm oral glucose tolerance test and pituitary MRI. However, we could not find any evidence of pituitary adenoma. We performed conventional and MR cerebral angiography for the evaluation of previous cerebral aneurysm(Fig. 5). They showed multiple fusiform dilatations of both middle cerebral arteries, posterior cerebral artery and left P2 segment. Aneurysms did not show, however, any impending rupture sign, and the patient strongly refused aneurysmectomy. We decided to make an observation.
Discussion
Carney complex, first described in 1985, is a multiple neoplasia syndrome that is composed of cardiac, endocrine, cutaneous, and neural tumors, as well as a variety of pigmented lesions of skin and mucosa.1)2) CNC is thought to be a familial disease, inherited in an autosomal dominant fashion, but some cases have been reported as sporadically occurring or genetically indeterminate.1) The diagnostic criteria for CNC have been recently reviewed(Table 1).3)4)
Our case was reported in 1984 as biatrial myxomas and in 1994 as recurrent left atrial and ventricular myxomas, and at those times, she had no other extracardiac myxomas and skin lesions. However, cutaneous myxomas, breast myxomatosis, and skin pigmentations were developed as time goes by. On the examination of her relatives, any characteristics of CNC could not be found. She was diagnosed as a sporadic form of CNC.
Cardiac myxomas are the most common component of CNC5) and this affect the four chambers of the heart. Forty one percent of CNC patients have multiple myxomas while 20% of patients have recurrent myxomas.5) Therefore, for the patients with CNC, if a history of cardiac myxoma is present, screening should be performed every 6 months by echocardiography.6) And if cardiac myxomas tend to be multiple and recurrent, we should consider the possibility of CNC, even other characteristics of CNC were not present at the time of diagnosis.
As is in this case, patients with left atrial myxomas usually present with signs of cardiac failure due to obstructed ventricular filling which causes dyspnea, pulmonary edema, and right heart failure.7) In at least half of the cases, cerebral arteries are affected, leading to embolic ischemic strokes. In contrast, the formation of intracranial aneurysms associated with left atrial myxomas is a less common phenomenon.8)
In the patients with CNC, cutaneous myxomas are presented in 40% of the patients with CNC,5) and common sites include eyelids, external ear canals, genital areas and nipples. Breast myxomas, bilateral, are also presented.6)
Clinically evident acromegaly is a relatively infrequent manifestation of CNC. However, asymptomatic elevation of GH and IGF-I levels, as well as subtle hyperprolactinemia, may be present in up to 75% of the patients.9)10) Also, in our patients, although IGF-1 and prolactin levels were slightly elevated, we could not find any evidence of pituitary adenoma on brain MRI.
Only a few cases of CNC have been reported in Korean medical literature.11-15) All of them were compatible with CNC at diagnosis.7)15-17) Our patient was diagnosed as multiple and recurrent cardiac myxomas until her second admission. But 11 years after resection, she was newly diagnosed as CNC by the presentation of cutaneous myxomas and skin pigmentations at intervals. Here, we present a rare case of CNC, diagnosed 11 years after resection of recurrent cardiac myxomas.




 XML Download
XML Download