

 PDF
PDF ePub
ePub Citation
Citation Print
Print



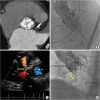
An 86-year-old female underwent transcatheter aortic valve implantation (TAVI) for severe aortic stenosis (AS) via a transfemoral approach. The aortic valve was a severely calcified bicuspid valve with fusion of the right and non-coronary cusps (Figure 1A). Therefore, a SAPIEN XT 26-mm valve (Edwards Lifesciences, Irvine, CA, USA) was implanted using a 1-mL-under balloon volume (Figure 1B). Transthoracic echocardiography (TTE) showed no problem one day after TAVI, but predischarge TTE at 1 week revealed a continuous shunt from the aorta to right ventricle (Figure 1C, Supplementary Video 1) and the pulmonary blood flow (Qp)/systemic blood flow (Qs) was 1.1. Aortography showed blood flow from the aortic annulus to the right ventricle (Figure 1D, Supplementary Video 2). She had no symptoms and was discharged on foot at 19 days after TAVI. At 18 months after TAVI, she was doing well without heart failure.
The silent onset of annulus rupture is very rare. Most annulus ruptures are observed during the initial procedure, and the patient's hemodynamic status is extremely unstable.1) In our case, the patient was very stable and the complication was late-onset. The mechanism of this complication may be erosion between the implanted valve edge and the aortic wall.2) Especially when there is a bicuspid valve with fusion of the right and non-coronary cusp, we need to carefully think about the type of implanted valve and the method of implantation. In addition, we need to carefully observe the patient for iatrogenic shunt, and percutaneous or surgical closure may be needed if the condition of the patient gets worse.

 XML Download
XML Download