

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiovascular implantable electronic devices (CIED) are extensively employed for arrhythmia and congestive heart failure.1) Simultaneously, there has been an associated increase in rate of CIED infections.2) CIED infections, frequently complicated by formation of vegetations on the intracardiac aspect of the leads and adjoining structures, including valvular leaflets, are associated with significant morbidity and mortality.3)4) In every single patient with CIED infections, complete device and lead removal with antimicrobial therapy is recommended.5) However, the extraction of chronically implanted transvenous lead systems remains a complex procedure and is associated with considerable morbidity and mortality.6) Sometimes, there is fragmentation of leads which leads to failure of extraction of all of pacing leads.7) The fate of remnant lead materials is still controversial. A study8) suggested that the extraction of an entire lead might not be necessary, if the lead could be totally separated from an infected pocket. Meanwhile, several studies reported that the intracardiac portion of a lead might be colonized even in cases limited to localized pocket infections.9)10)11) In addition to the aspect of CIED infections, remnant lead fragments may cause mechanical complications such as embolization into the pulmonary arterial bed.7)12) This report describes cases of five patients with remnant lead tips after lead extraction for CIED infections and managed only by administration of antibiotics. This study was approved by the Institutional Review Board of Yonsei University Hospital.
Case
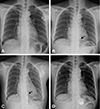
Among 86 patients, who underwent lead removals for CIED infections between January 2000 to June 2015, a transvenous and a surgical lead removal was performed in 84 (98%) and two (2%) patients, respectively. Five patients had remnant lead tips (Fig. 1). The clinical features of these five patients are described below.
Patients with localized pocket infections
Case 1
A 93-year-old female was admitted for skin erosion at the site of the generator pocket (Patient 1 in Table 1-1). The patient had undergone a permanent dual chamber (DDD) pacemaker implantation 10 years back for symptomatic sick sinus syndrome.
There was no evidence of a systemic infection. The patient underwent a transvenous lead removal initially using the direct traction and traction/counter-traction method with a locking stylet. The lead tip separated from the right ventricle (RV) lead during the extraction procedure (Patient 1 in Table 1-2). Two weeks after the extraction, the remnant RV lead tip embolized into the right middle pulmonary artery (Fig. 2A). There was no evidence of a pulmonary infarction or infection. During a 4-year follow up study, no adverse events were reported.
Case 2
A 43-year-old male was referred for the left-sided generator exposure (Patient 2 in Table 1-1). The patient had Eisenmenger syndrome and right heart failure. The patient had undergone a DDD pacemaker implantation 31 years back for complete atrioventricular block, via the left subclavian vein. Due to a lead fracture of left sided DDD pacemaker, an atrial synchronous, ventricular demand (VDD) pacemaker was newly implanted via the right subclavian vein 10 years back. He was treated with oral antibiotics at the referring hospital for a week.
We tried a transvenous lead extraction of the DDD pacemaker. The left sided RV lead was separated at the middle part, and almost 10 cm of the RV lead was still present. To remove the remaining lead, transfemoral traction with a snare was used (Patient 2 in Table 1-2). However, we failed to remove the tip of the RV lead (Fig. 2B). Because of the unstable condition due to severe pulmonary hypertension, the procedure was terminated. The patient did not show any further evidence of infection and we decided to maintain the right sided VDD pacemaker. During 23-months of follow up, the patient has shown no evidence of infection or complications.
Patients with systemic infections
Case 3
A 77-year-old male was admitted for fever (Patient 3 in Table 1-1). The patient had undergone a DDD pacemaker implantation 18 years back for complete atrioventricular block. Transthoracic echocardiogram (TTE) revealed multiple vegetations (2.0 cm maximum) attached to the RV lead. The patient initially underwent a surgical lead extraction, considering large vegetations. The RV lead was not completely removed because of severe adhesion to the leaflet and chordae of the tricuspid valve. The proximal part of remaining RV lead in the left subclavian vein was removed by a transvenous approach (Patient 3 in Table 1-2). However, the tip of RV lead was left behind (Fig. 2C). A new pacemaker was implanted via the right subclavian vein 14 days after the device removal (18 days after the blood cultures were confirmed to be negative). During 26-months of follow up, the patient has shown no evidence of infection or complications.
Case 4
A 69-year-old male was admitted for fever and chills (Patient 4 in Table 1-1). The patient had undergone a VDD pacemaker implantation 8 years back for symptomatic tachy-brady syndrome. TTE revealed vegetation (0.9×0.6 cm) attached to the right atrium (RA) lead and severe tricuspid regurgitation (TR). The patient had to undergo a surgical lead extraction for simultaneous surgical correction of severe TR. The VDD lead was not completely removed because of severe adhesion to the chordae of the tricuspid valve. The proximal part of remaining VDD lead in the left subclavian vein was removed by a transvenous approach via the left subclavian vein (Patient 4 in Table 1-2). However, the VDD lead tip was still left behind (Fig. 2D). A pacemaker was implanted epicardially at the time of the initial surgical removal. There was no evidence of any resurgence of the infection after the completion of the antibiotic therapy, at the 36-months follow up.
Case 5
A 54-year-old female was admitted due to continuous fever for a month (Patient 5 in Table 1-1). The patient had undergone a ventricular demand pacing (VVI) pacemaker implantation for complete atrioventricular block via the right subclavian vein 22 years back. Eleven years after initial implantation, the right-sided generator was removed for the generator exposure and a new VVI pacemaker was implanted via the left subclavian vein (Fig. 3A). At the time of admission, transesophageal echocardiogram (TEE) showed multiple and large (2.3 cm maximum) vegetations attached to the pacemaker leads, septum, and tricuspid valve. We tried to remove the pacemaker leads by the traction/countertraction method with a locking stylet. The left sided pacemaker lead was completely removed. The ventricular lead of the right sided pacemaker was fractured and removed by a transfemoral traction method with the aid of a snare kit (Patient 5 in Table 1-2). Unfortunately, the ventricular lead tip fragmented off and was left behind in the RV apex (Fig. 3B). A new VVI pacemaker was implanted three months after the lead extraction (Fig. 3C). A month after the new pacemaker implantation, the patient was admitted for fever. TEE showed presence of a new vegetation attached to the newly implanted lead. The vegetation and the lead were removed by open heart surgery, and an epicardial pacemaker was newly implanted (Fig. 3D).
Discussion
Because of the concerns over colonization and the higher risk of recurrence, the mainstay of CIED infection management has been established as the complete removal of the entire implanted device system in patients with device-related endocarditis, and also with only localized pocket infections.13)14)15) Although the extraction procedure has matured into a defined art, the physicians still fail to remove all the components of an implanted system by the transvenous approach and even by the surgical approach. In patients with pocket infections, Love et al.8) reported that extraction of an entire lead might not be necessary if the lead could be totally separated from an infected pocket. Also, a case of curing the infection through antibiotic administration alone has been reported.16) However, the outcomes and optimal management of device-related endocarditis with retained material have not been elucidated. We experienced cases of two locally infected patients and three endocarditis patients with retained lead fragments after the device removal. All the remaining parts of their devices were RV lead tips. Considering that most CIED infections are due to staphylococcal species and some of the species would be methicillin resistant, vancomycin (Patients 2, 3, and 5) and teicoplanin (Patients 1 and 4), were administered to the patients as initial empirical antibiotics until the culture results were revealed. In the patients whose infections were limited to the pocket site (Patients 1 and 2); we continued the antibiotic treatment for over seven days with parenteral agents and for a total of 14 days. In patients with systemic infections, we continued the parenteral antibiotic therapy for at least 4 weeks. Neither locally infected patients nor systemically infected patients experienced any relapse of the infection during a median of 26-month follow up (range 5-48 months). For the CIED infection, in cases with remaining fragmented lead tips, we suggest that a conservative management with a sufficiently long, proper antibiotic treatment can be considered.
Only 1 out of 5 patients (Patient 1) had complications caused due to retaining material in our series. Development of pulmonary embolization of the remnant lead tip occurred, but there was no evidence of infection or pulmonary infarction, and the patient did not undergo any additional treatment during 48-months of follow-up.
Three patients (Patients 3, 4, and 5) underwent new pacemaker reimplantations and all those patients had systemic infections initially. Two patients showed no relapse of infections or other complications after the reimplantation, suggesting that the remaining lead fragments were not an absolute contraindication for the implantation of a new intracardiac device. However, Patient 5 had relapsing fever a month after implantation of a new pacemaker. The patient had to undergo open heart surgery for complete removal of the remnant lead.
In conclusion, in the case of patients with remnant lead tips after a hardware removal for a CIED infection and with device-related endocarditis, conservative treatment with antibiotics without the retrieval of material can be a safe and effective way. One of five patients with retained lead tips in our series experienced pulmonary embolism, but neither there was an evidence of an infection nor occurrence of pulmonary infarction. Only one of five patients experienced resurgence of an infection.




 XML Download
XML Download