

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A 69-year-old woman diagnosed as having end-stage dilated cardiomyopathy had undergone partial left ventriculectomy (PLV) in 1996. This is the first reported case of PLV (Batista procedure) in Korea.1) She was doing well under the New York Heart Association class II diagnosis in November 2009 and had received 3-dimensional (3D) echocardiography for the evaluation of cardiac function.
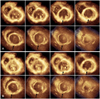
Full volume 3D echocardiography (Philips Medical, IE33, Bothell, WA, USA) of the heart showed a dilated left ventricle (LV) and gave a more accurate LV ejection fraction and time-volume curve during one cardiac cycle (Fig. 1) compared with 2D echocardiography which is inevitably done in different cardiac cycles (Fig. 2). LV end-diastolic and end-systolic volume index were 109.3 mL/m2 and 88.79 mL/m2, and ejection fraction was 18.8% in 3D echocardiography. We could see detailed morphology of the endocardium and myocardium of the LV after PLV (Fig. 3). This is the first report of 3D echocardiographic findings of the LV after long-term follow up (of 13 years) from PLV. 3D echocardiography is a useful non-invasive method for the evaluation of cardiac function after LV volume reduction surgery.
PLV, which was introduced by Batista in 1995, is one surgical alternative treatment for end-stage heart failure.2) Resection of the myocardium not only decreases wall stress according to Laplace's law, but may improve stroke volume for sufficiently dilated and depressed ventricles. Using these operative techniques to alter the shape of the LV, in combination with optimal medical management for heart failure, improves survival.3) Although a favorable outcome has been reported in selected patients, this method is currently not recommended for treatment of heart failure because of high surgical failure rates.4)5) Here, we report 3D echocardiographic findings of long-term survival of a patient who had undergone a Batista procedure 13 years ago.


 XML Download
XML Download