

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The classic presentation of rhabdomyolysis includes myalgias and pigmenturia due to myoglobinuria in association with elevated concentrations of serum muscle enzymes. The common causes include crush injuries, prolonged immobilization, seizures, severe infections and drug toxicity.1) Statins are a well-known cause of rhabdomyolysis, and exercise may increase the risk of statin-induced rhabdomyolysis.2) Moreover, some cases associated with sauna exposure have been reported, albeit rarely.3)4)
Case
A 63-year-old woman presented with myalgia and muscle weakness in both lower extremities, and this had begun 5 days prior to admission. She had been taking simvastatin (40 mg/day) for over 6 years due to dyslipidemia, and she had never experienced relevant symptoms. She denied alcohol use and she had not previously exercised regularly. For her personal history, she had taken a sauna for about 4 hours per day for 20 years with the goal of relieving she unusual chronic fatigue. One week prior to admission, she had started a weight loss program that included running exercise in the sauna for about 30 minutes per day to exhaustion, and she had stayed an additional 1-2 hours more in the sauna than she previously had. Two days later, she had developed myalgia and muscle weakness in both lower extremities. She reported and showed no burn injuries from her time in the sauna.
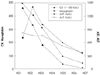
On physical examination, she was 165 cm tall and weighed 66 kg, and she was in no distress; she had no fever or abnormal findings other than muscle tenderness in the lower extremities. The serum creatine kinase level was 45,990 IU/L (8 months prior, it was 407 IU/L), the myoglobin level was 229 ng/mL and the creatine kinase-MB (CK-MB) was greater than 80 ng/mL. The aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were elevated to 1,487 IU/L and 820 IU/L, respectively, but the other liver function tests were within normal limits, (Fig. 1) and the hepatitis viral markers were nonspecific. The urine color was dark-brownish, and the urinanalysis result was +3 for blood by dipstick analysis, but the microscopic examinations for red blood cells (RBCs) and white blood cells (WBCs) were within normal limits. The serum lectrolytes, urea, creatinine levels and thyroid function tests were normal. The electrocardiogram was normal. With the diagnosis of rhabdomyolysis, intravenous hydration with discontinuation of simvastatin was proscribed to prevent renal failure. Her symptoms were improved the next day, and the creatine kinase level decreased to 33,360 IU/L. The patient was discharged with minimal residual muscle weakness one week after discontinuing the simvastatin, exercise and sauna use. At discharge, the creatine kinase level was 914 IU/L and the AST level was 132 IU/L.
Discussion
The usually prescribed doses of statins are safe, and severe complications such as rhabdomyolysis are rare.5)6) Particularly, the incidence of statin monotherapy-induced rhabdomyolysis (except for cerivastatin) is very low, with the incidence rate per year of therapy being only 0.0042%.7) However, previous studies have shown that there is a higher incidence of statin-induced rhabdomyolysis when statins are used along with drugs that affect the cytochrome P450 3A4 system, i.e., fibrate, nicotinic acid, cyclosporine, macrolide antibiotics and others.8) In our case, the patient had been taking simvastatin for 6 years, and she had not taken any drugs that interact with the statin metabolism during that time.
Heat stroke is another well known cause of rhabdomyolysis. Exertional heat stroke is an extreme form of exertional hyperthermia in which muscular exertion during hot, humid weather results in an excessive storage of heat.9) The mechanisms for rhabdomyolysis in this condition are hypovolemia and a total body potassium deficit due to excessive sweating. The potassium deficit is aggravated by the increased renin-aldosterone activity due to hypovolemia.4) The role of potassium in the regulation of skeletal muscle blood flow appears to be pathogenetically important in rhabdomyolysis. The cellular release of potassium is impaired by potassium depletion, and as a result, the decreased blood flow results in cramps, ischemic necrosis and rhabdomyolysis.10) There have been several case reports in which the occurrence of rhabdomyolysis was associated with sauna exposure.3)4) These investigators speculated that sauna use may activate the same causation mechanism as heat stroke does. We think this is plausible in our case. The proposed risk factors for statin-induced rhabdomyolysis are an advanced age (>80 y), a small body frame and frailty, renal or hepatic dysfunction, thyroid disorder, hypertriglyceridemia, metabolic muscle disease, alcohol and heavy exercise.8) There was one case report in which long-term statin treatment caused rhabdomyolysis following severe unaccustomed exertion.11) These investigators noted that statins amplified the muscle damage that was caused by intense exertion. In the studies concerned with statins and exertion-induced muscle damage, the patients receiving lovastatin had 62-77% higher creatine kinase levels after exercise compared to those patients on placebo, showing that statins increase exercise-induced muscle injury.12) In our case, the patient was in a state that was vulnerable to rhabdomyolysis due to sauna exposure and her statin medication. In this situation, the patient did unaccustomed exercise, and we speculate that this triggered the rhabdomyolysis.
Rhabdomyolysis is considered to be one of the most important complications that occurs in the population taking statins. Our patient developed rhabdomyolysis due to the combined use of statins, unaccustomed exercise and sauna exposure. We suggest that physicians should advise their patients who are taking statins to be aware of the risk factors for rhabdomyolysis, and to avoid any other medications or personal activities that would increase their risk for developing rhabdomyolysis.
 XML Download
XML Download