

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
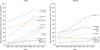
Cancer has been a leading cause of death in Korea since 1983, when official national mortality statistics were initially published.1 Approximately 200,000 new cancer patients have been identified every year through national and regional cancer registries,2 and more than 78,000 cancer deaths were reported in 2016.3 Although the actual figures vary widely depending on the primary sites, the crude (CR) and age-standardized incidence rates (ASR) of all types of cancer have been increasing in both genders during the most recent 17 years (Fig. 1). The ASR of cancer in 1999 was 219.9 per 100,000 persons (291.9 and 173.3 in men and women, respectively), and this figure increased to 258.9 per 100,000 persons (291.7 and 241.1 in men and women, respectively) in 2015 (Table 1). In fact, the national burden of cancer has increased further due to the aging population in Korea. The age-standardized disability-adjusted life years (DALY) for cancer between 1990 and 2013 decreased by 32%, but cancer is still ranked second among the 12 major disease categories in this regard.4 Indeed, Korea is a country with a high male smoking rate, about 40% in 2012.5 According to the Korean National Health and Nutrition Examination Survey (KNHANES) and the Korean Youth Risk Behavior Web-based Survey (KYRBWS), the age-standardized current smoking rate among adult men (≥19 years) slightly decreased from 47.7% in 2004 to 42.1% in 2013, and recent smoking rates among adolescents were 14.4% in male and 4.6% in female students in 2013.6 The prevalence of grade 2 obesity (body mass index, BMI ≥30 kg/m2) in KNHANES increased 3.3-fold in men and 1.4-fold in women from 1998 to 2014.7 The prevalence of cancer-causing infectious diseases, such as Helicobacter pylori (H. pylori), hepatitis B virus (HBV), hepatitis C virus (HCV), and human papillomavirus (HPV), remain high in Korea.89101112 As a result, the proportions of all cancers in Korea attributable to infection were 21.2% in terms of cancer incidence and 24.7% in terms of cancer-related deaths13; the population-attributable fractions (PAFs) were higher than those for all cancer cases in the world and for those in developed countries,14 and they were similar to those for low-and middle income countries.15
This paper presents an up-to-date review of trends in cancer incidence, mortality, and survival rates and relevant risk factors for cancer for 11 major cancer sites in Korea. All incidence and survival data that is used in this paper was extracted from previously published papers based on the database of the Korea National Cancer Registry and mortality data were obtained from Statistics Korea.3 Information on the status of cancer risk factors is cited from various types of national health surveys, including KNHANES and KYRBWS.
INCIDENCE, MORTALITY, AND SURVIVAL
1. Gastric cancer
Gastric cancer is the most common cancer in Korea, it was the most common cancer in men and the fourth most common in women in 2015. The number of new gastric cancer cases increased from 20,870 in 1999 (20.7% of all cancers) to 29,207 in 2015 (13.6% of all cancers).2 Although the ASR per 100,000 persons decreased from 43.6 in 1999 to 33.8 in 2015,2 Korea still has the highest ASR for gastric cancer in the world.16 The gastric cancer incidence rate changed only slightly between 1999 and 2011, and it began to decrease more sharply in both sexes in 2012. The estimated annual percent changes (EAPCs) during 1999–2011 were −0.3% both in men and women, and the EAPCs during 2011–2015 were −6.2% and −5.1% in men and women, respectively (Table 2). Consistent with global trends, the declining incidence in gastric cancer is attributable primarily to a decrease in the incidence of non-cardia cancer.171819 Between 1999 and 2014, the proportion of gastric cancer cases in the cardia/fundus increased only slightly (5.9% to 7.1%), but the proportion in the entire body increased even more (35.3% to 43.2%).20 In terms of histologic type, according to a nationwide survey, moderately differentiated tubular adenocarcinoma (30.2%) was the most common, followed by poorly differentiated (28.5%), signet ring cell (18.1%), and well-differentiated (11.5%) types.21
Gastric cancer is the fourth most common cancer-causing death in Korean population. In 2016, 8,264 persons (5,318 men and 2,946 women) died from gastric cancer, and the crude mortality rate per 100,000 persons was 16.2 (20.8 in men and 11.5 in women).22 The gastric cancer mortality rates (per 100,000) were 13.0 in 2012 and 9.7 in 2014 (15.1 among men and 5.7 in women in 2014) after adjustment for the global population; this was similar to the figure for Japan (12.4) but six-fold higher than that for the United States (US) (2.0) in 2012.1622 The mortality rates both globally and in Korea have decreased substantially over the last two decades.19 The recent negative EAPCs during 2000–2009 were about −26% in all age groups and −14% in those aged 35–64 years.19 The decreasing trends in the incidence of deaths primarily related to gastric cancer may reflect changes in exposure to the main risk factors for this type of cancer, such as H. pylori, across the population. A significant decreasing trend in the prevalence of H. pylori was reported in a nationwide multicenter study. The respective seroprevalences of H. pylori were 66.9%, 59.6%, and 54.4% in 1998, 2005, and 2011.8 The expanded national gastric cancer screening program using upper endoscopy may have also contributed to the reduction in gastric cancer mortality via lowering the risk of being diagnosed at an advanced stage23 and by applying H. pylori eradication treatment after endoscopic diagnosis. According to a nationwide nested case-control study of 54,418 gastric cancer cases and 16,584,283 cancer-free subjects aged 40 years and older, the overall odds ratio (OR) and 95% confidence intervals (CI) for dying from gastric cancer were 0.79 (0.77–0.81) among ever-screened subjects compared to never-screened subjects. In terms of screening modalities, an upper gastrointestinal series (UGI) was not significantly associated with reductions in mortality. However, endoscopic screening significantly reduced gastric cancer mortality in a dose-response manner. The ORs (95% CIs) for gastric cancer deaths were 0.60 (0.57–0.63), 0.32 (0.28–0.37), and 0.19 (0.14–0.26) among those who had undergone one, two, and three or more lifetime endoscopic screenings, respectively.24
The 5-year net survival rate (NSR) of gastric cancer improved from 48.6% in 2000–2004 to 68.9% in 2010–2014, the highest among 71 countries worldwide.25 During 2010–2014, the 5-year relative survival rate (RSR) in men (75.3%) was higher than that in women (72.7%) (Fig. 2).22
The Korean diet, including their high intake of salty and spicy foods and higher intake of cooked foods than fresh vegetables, are believed to be one of the most important causes of the high incidence of gastric cancer in Korea.26 The high seroprevalence of H. pylori is also believed to be responsible for the high incidence of gastric cancer. The prevalence of H. pylori in Korean adults was greater than 80% in the 1980s,12 and decreased to less than 55% in 2011.8 Whether eradication of H. pylori will reduce the incidence of gastric cancer in the Korean population remains controversial. A recent hospital-based retrospective cohort study of 38,984 subjects reported the protective effect of H. pylori eradication on the occurrence of gastric cancer. The cumulative risk of gastric cancer is significantly higher in patients with non-eradicated H. pylori than in those who have undergone eradication (OR 2.73, 95% CI 1.50–4.98), and there was no significant difference between the eradication group and those who were H. pylori-negative (OR 1.51, 95% CI 0.693.29).27
2. Colorectal cancer
In Korea, colorectal cancer (CRC) is the second most common cancer among men and the third most common cancer among women, and the most common cancer among women aged 65 years and older.2 The number of new cases in 2015 (15,911 cases in men and 10,879 cases in women) was more than double that (9,714 cases) in 1999 (5,310 cases in men and 4,404 cases in women).228 The ASR of CRC among men was 27.0 in 1999, and it increased to 50.2 in 2009 (EAPC, 6.6%). The ASR for women was 17.2 in 1999 and 26.9 in 2009 (EAPC, 5.1%). In terms of subsites, distal colon cancer consistently showed the highest EAPCs in most age groups of both men and women.28 The proportion attributable to rectal cancer was 43.4% in 2014 (45.8% in men and 39.8% in women), which was much higher than that in the US (28%; 32% in men and 24% in women).29 This increasing trend of CRC has been declining since 2011. The EAPC during 1999–2010 was 6.0%, but it reversed by −4.9% in 2010–2015 (Table 2). Based on linear regression analysis and projections, the predicted ASR in 2017 was 29.3 (37.6 in men and 22.4 in women).30 The national cancer screening program for CRC is also considered an important contributor to the increase in CRC.31 However, a multiethnic study in the US found that Korean men were the only Asian (Japanese, Chinese, Filipinos, Vietnamese, and South Asians) immigrants in the US to experience a significant increase in the incidence of CRC between 1988 and 2007.32 Several problematic lifestyle factors, such as frequent alcohol consumption,33 higher saturated fatty acid intake,34 and physical inactivity related to obesity, may have also contributed to the increasing trend.35 Frequent meat consumption was associated with the risk of proximal colon cancer in men (p for trend=0.005) and of rectal cancer in women (p for trend= 0.002).36 Risk factors for CRC differed by subsite and sex. Proximal colon cancer in men and rectal cancer in women were associated with frequent meat consumption.36
The fact that CRC along with anal cancer has been known to cause deaths as the third most common cancer in Korea; it was the fourth most common in men and the second most common in women in 2016. In women, the crude mortality rate of CRC (14.6 per 100,000) was higher than the gastric cancer mortality rate (11.5). However, CRC-related mortality was higher in men (18.4) than in women (14.6), and the age-standardized mortality in men (13.8) was about twice as high as that in women (7.5).22 The decreasing trend in CRC mortality initially occurred in younger individuals as well as in other East Asian countries37 and reflected birth cohort effects.38 The birth cohort effect implies that the decreasing CRC mortality rates may be due to earlier detection and advances in treatment, especially in younger populations. The CRC screening program may have initially increased the incidence, but it has been shown to reduce the incidence over time.39
The survival rate for CRC in Korea has improved in both sexes and all subsites between 1993 and 2010.40 Distal colon cancer, which was associated with more favorable survival rates than proximal colon or rectal cancer, is especially common among younger individuals.40 The 5-year NSR from 2010 to 2014 was 71.8% for colon and 71.1% for rectal cancer.25 Another study reported that the 5-year RSR of CRC in 2010–2014 was 76.3% (78.1% in men and 73.4% in women). The EAPCs of the 5-year RSRs for CRC from 1993–1995 to 2011–2015 was 21.5% (22.7% in men and 19.4% in women).2
3. Lung cancer
Presently, despite previously known statistics, lung cancer is the fourth most common cancer effecting Korean population; it was the second most common in men and the fifth most common in women, with an ASR of 26.4 per 100,000 (42.3 in men and 14.3 in women) in 2015 (Table 1). In men, the ASR of lung cancer is the second highest, after gastric cancer, and it is the most common cancer among men aged 65 years and older.22 In total, 24,267 incident cases (17,015 men and 7,252 women) and 17,399 deaths (12,677 men and 4,722 women) were identified in 2015. The mortality to incidence ratio (MIR) of lung cancer is 0.72 (0.75 in men and 0.65 in women). The MIR is higher than that for other major cancer sites but lower than the average value for all Organization for Economic Cooperation and Development (OECD) countries (0.80).41 In Korea, the incidence of lung cancer began a declining trend in 2012, especially in men, with an EPAC of −1.8% (Table 2). The decline was not significant in women.22 In terms of histologic types, adenocarcinoma has been the most common type since 2011, and its incidence increased in 1999–2012, with an EAPC of 4.1%. Otherwise, squamous cell carcinoma and small-cell carcinoma showed decreases in both sexes, with EAPC values of −1.7% and −0.5%, respectively.42
Lung cancer is a leading cause of cancer-related death in Korea, and the number of deaths from lung cancer has increased since 1983 in both sexes. In total, 17,963 deaths attributable to lung cancer (13,324 men and 4,639 women) occurred in 2016, accounting for 6.3% of all deaths in 2016. The crude mortality of lung cancer in 2016 was 35.1 (52.2 in men and 18.1 in women), and the age-adjusted mortality was 21.9 (38.9 in men and 9.5 in women).3 However, the lung cancer mortality rates started to decline in 2002, with an EAPC of −2.1% (−2.5% in men and −1.5% in women).242 This trend may be explained by the birth cohort effect and changes in smoking patterns. Indeed, tobacco control policies were first implemented in 1986, and the National Health Promotion Act, which contained several strengthened tobacco control policies, was implemented in 1995. Tobacco smoking is the most important modifiable risk factor for cancer identified thus far, as it is estimated to be responsible for 20.9% of all incident cancer cases and 32.9% of all cancer-related deaths among Korean male adults.43 The PAFs of smoking for cancer incidence and cancer deaths in women were lower than those in men, and the respective PAFs of smoking were 2.1% and 5.2% in women.43 The smoking rate has continuously declined, from 72% in 1992 to 42% in 2013 in adult men, but it has not significantly changed in women.6
The survival rate of lung cancer patients has improved continuously during the last two decades. The 5-year RSR in 1993–1995 was 11.3%, and it was 26.7% in 2011–20152; the 5-year NSR during 2010–2014 was 25.1% (95% CI 24.8–25.4%).25 Improved access to various clinical modalities, such as target agents, surgery, and sophisticated diagnostic tools, may be associated with the increasing upward trend in the survival rate of lung cancer patients.
4. Liver cancer
Liver cancer is the sixth most common cancer, and it is the fourth most common in men and the sixth most common in women; it is also the second most common cause of cancer-related deaths in Korea.2 In total, 15,757 incident cases (11,732 cases in men and 4,025 cases in women) were identified in 2015 and 11,001 deaths (8,044 deaths in men and 2,957 deaths in women) were reported in 2016, respectively. The ASR per 100,000 was 18.24 (29.5 in men and 8.2 in women) in 2015 and the age-standardized mortality per 100,000 was 14.3 (23.5 in men and 6.5 in women) in 2016, respectively.23 The number of cases and CRs of primary liver cancer increased from 1999 to 2011, and the peak number of cases was 16,714, with a CR of 33.4. However, the ASRs showed a decreasing trend during recent decades, moving from 27.9 in 1999 to 18.2 in 201444 The EAPCs of the incidence of liver cancer in 1999–2010 and 2010–2015 were −1.7% and −4.6%, respectively (Table 2).2
Mortality from liver cancer has also decreased since 2002 in both sexes. The EAPC of liver cancer mortality during 2002–2015 was −3.6% (−3.7% in men and −3.7% in women) (Table 3).2 In 2014, the peak age group was 50–59 years (27.3%), followed by 60–69 years (25.2%) and 70–79 years (24.8%).44
The 5-year RSR of liver cancer was 27.2% (95% CI 26.8–27.7) among cases diagnosed in 2010–2014, which was higher than the comparable figures for 2005–2009 and 2000–2004: 22.4% and 15.3%, respectively.25 The EAPC of the 5-year RSR was 22.9% (24.2% in men and 18.6% in women) during 1993–2015.2
The risk factors for liver cancer, such as the hepatitis B (HBV) and C (HCV) viruses and heavy alcohol consumption, are main causes of hepatocellular carcinoma (HCC). In Korea, HBV, HCV, and alcohol consumption accounted for 62–75%, approximately 10%, and 2.4–10.9%, respectively, of HCC cases.44 A recent nationwide survey, KNAHNES 2012–2014, reported that the prevalence of HBV, defined as HBV surface antigen carriers, and HCV, defined as anti-HCV antibody carriers, were estimated at 2.9% and 0.62% (95% CI 0.49–0.78%), respectively. The prevalence of HCV was higher in women (male-to-female ratio: 1.38) and increased with age in both sexes. The positive rate of HCV RNA in those who were anti-HCV-positive was 32.5% in this study.41
5. Breast cancer
Breast cancer is the second most common cancer in Korean women, following only by thyroid cancer. The number of cases, CR, and ASR in women have been rapidly increasing since 1999. The number of breast cancer cases increased from 6,025 (5,703 invasive cases and 322 carcinomas in situ) in 1999 to 21,402 cases (18,304 invasive and 3,098 in situ) in 2014. When standardized with the 2000 Korean standard population, the respective ASRs of in situ, invasive, and total breast cancer increased from 1.4, 24.5, and 26.1, respectively, in 1999 to 9.6, 54.4 and 63.9 per 100,000, respectively, in 2014; the EAPCs were 13.5%, 5.5%, and 6.1%, respectively. The EAPC of carcinoma in situ was more than twice as high as that of invasive breast cancer in 1999–2014.45 In 2014, the most cases occurred in women aged 40–49 years (7,602 cases, 35.4% of total cases), and the second most occurred in those aged 50–59 years (6,550 cases, 30.5%). The mean age at diagnosis slightly increased, from 47 years in 2002 to 50 years in 2014. The proportion of postmenopausal women with breast cancer increased from 40.6% in 2002 to 52.1% in 2014. The proportion of estrogen receptor- and progesterone receptor cases also increased, from 58.2% and 50.7% in 2002 to 74.1% and 62.4%, respectively, in 2014.45 In 2012, the most common histologic types of breast cancer were invasive ductal carcinoma (83.1%), followed by ductal carcinoma in situ (12.0%).46
A total of 2,472 persons (2,456 women and 16 men) died from breast cancer in 2016. The crude mortality rate per 100,000 in women was 6.9 in 2016,3 and the age-standardized mortality rate (standardized with the world population) was 5.5 in 2015. Mortality gradually increased from 1999 through 2015, with an EAPC of 1.4% (Table 3).2
The 5-year RSR for all-stage breast cancer increased from 79.5% in 2000–2004 and 84.0% in 2005–2009 to 86.6% in 2010–2014.25 The stage-specific 5-year and 10-year survival rates among the 109,979 breast cancer cases diagnosed during 2001–2012 were 96.6% and 92.7% for stage I, 91.8% and 84.8% for stage II, 75.8% and 63.4% for stage III, and 34.0% and 22.2% for stage IV, respectively.45
A Westernized lifestyle, including a Westernized diet and infant feeding patterns, early menarche or late menopause, delayed marriage, and having fewer children at an older age, might be associated with the increasing trend in breast cancer in Korean women.46
6. Thyroid cancer
Following the global trend in direction but surpassing it in rate, the incidence of thyroid cancer has rapidly increased in Korea during recent decades. Thyroid cancer has been the most frequently diagnosed cancer in Korean women since 2005,47 and it was the sixth most common cancer in men in 2015, with an estimated 25,000 cases and 350 deaths. During 2012–2013, the incidence of thyroid cancer was even higher than that of prostate cancer in men. The incidence of thyroid cancer began to decrease in 2013 and 2012 in men and women, respectively,2 but these rates remain the highest in the world for both sexes.16 The ASRs per 100,000 persons, men, and women increased from 6.3, 2.1, and 10.4, respectively, in 1999 to 35.2, 15.1, and 55.6, respectively, in 2015. There were 25,029 (5,386 men and 19,643 women) thyroid cancer cases in 2015, accounting for 11.7% of cancer cases (4.8% in men and 19.4% in women).2 The most common histologic subtype of thyroid cancer is papillary cancer, and this is related to increasing thyroid cancer screening in Korea.48 The proportion of screening-detected thyroid cancers increased from 15.0% in 1999 to 59.1% in 2008. During the same period, the number and proportion of papillary carcinomas increased from 779 (87.4%) to 2,478 (97.2%), but the ASRs of other histologic types, including follicular, medullary, and anaplastic carcinoma, decreased from 62 (7.0%) to 45 (1.8%), from 43 (0.7%) to 11 (0.4%), and from 26 (0.5%) to 5 (0.2%), respectively.49 Despite this increasing trend, the thyroid cancer mortality rate has decreased since 2003. The EAPC of thyroid cancer mortality from 2003 to 2015was −4.2%, and the age-standardized mortality from thyroid cancer was 0.3 per 100,000 persons (0.3 in men and 0.5 in women) in 2015.24 In 2016, there were 346 deaths (104 men and 242 women) attributable to thyroid cancer, accounting for 0.4% of cancer-related deaths (0.2% in men and 0.8% in women); 283 of these cases (81.8%) were aged 65 years and older. The crude mortality per 100,000 persons has remained almost unchanged, between 0.7 and 0.8, since 2000.3 It is almost certain that thyroid cancer screening is the primary contributor to the increased incidence of this disease, especially papillary carcinoma; however, no association was found with the decreasing mortality rates.48
The 5-year RSR for thyroid cancer was over 100% in the period 2011–2015 in both sexes, which means that it was higher than the observed 5-year survival rate among the general population. The 5-year RSR increased from 94.2% in 1993–1995 to 100.3% in 2011–2015.2
7. Cervical cancer
Cervical cancer is the seventh most common cancer and the third leading cause of cancer-related deaths among Korean women. In 2015, 3,582 cases, 3.5% of all cancer cases, were newly diagnosed; the CR and ASR were 14.1 and 9.1, respectively. Since 1999, the incidence of cervical cancer has decreased steadily, from 16.3 in 1999 to 9.1 in 2015, with an EAPC of −3.7%.2 However, the trends in incidence rates differ by age group and type of invasiveness. The age-specific incidence rate of cervical cancer showed a decreasing trend in all age groups except those younger than 30 years. The EAPCs of the age-specific incidence rate from 1993 to 2012 were 5.6% (95% CI 2.9–8.3%) and 2.5% (95% CI 1.4–2.5%) among 20–24-year-old and 25–29-year-old women, respectively.10 Additionally, the incidence of invasive cervical carcinoma (ICC) decreased but that of in situ increased. No significant trend in the incidence of ICC was observed in those aged 20–29 years.50 The peak age for the incidence of cervical cancer changed from 60–64 years in 1993–1997 to 75–79 years in 2008–2012. Cervical cancer is considered to be among the most preventable cancers because of its slow progression, the availability of screening, and widespread access to the HPV vaccine. In 2014, the rate of participation in the Korean nationwide cervical cancer screening program was estimated at 51.5% (95% CI 48.6–52.5%) among women aged 30 years or older according to data on National Health Insurance beneficiaries.51 The National Immunization Program against HPV directed at female adolescents of 12 years was launched in 2016. The estimated prevalence of HPV among healthy Korean women ranged from 16.7% to 27.8% in nationwide studies. HPV 54 was most frequent type of low-risk HPV, and HPV 53 was most common among the 19 high-risk HPV strains.5253 HPV 16 and HPV 18 are major causes of ICC and precancerous lesions in the cervix, accounting for approximately 70% of the ICC and 50% of the intraepithelial neoplasia 2/3 cases.54 The risk of squamous cell carcinoma in the cervix is known to be about 400- and 250-fold higher in women infected with HPV16 and HPV18, respectively, than in healthy individuals.11
The number of deaths from cervical cancer peaked in 2003 (n=1,111), and 897 deaths were reported in 2016, accounting for 2.9% of all cancer-related deaths. The crude and age-standardized mortality rates based on the 2000 Korean standard population were 3.5 and 2.3, respectively, per 100,000 persons in 2016.3 The age-standardized mortality rate of cervix cancer has decreased since 2003, with an EAPC of −4.9% during 2003–2015 (Table 3).
8. Prostate cancer
Prostate cancer is the fifth most common cancer among Korean males. Continuous incline of prostate cancer were seen from 1,437 cases in 1999 to 10,212 cases in 2015. Prostate cancer accounted for 9.0% of all cancer cases among men, and the CR was 40.1 per 100,000 persons. The ASR of prostate cancer peaked in 2011, with 27.9 per 100,000 persons, and it decreased slightly, to 25.4, in 2015.2 The age-specific incidence rate was highest in those aged 80–84 years, followed by those aged 75–79 years. However, the fold-increase rate in prostate cancer from 1999 to 2012 was only 1.5 in men aged 80–84 years, but it increased more than four-fold in men aged 55–59, 60–64, and 65–69 years.55 Parallel to the global pattern, the increase in screening with prostate-specific antigen (PSA) may be the most important contributor to the recent increasing trend in the incidence of this disease, but the increase in the aging population and spread of a Westernized lifestyle, including an animal-protein rich diet, may have also contributed.56 A hospital-based study found that the proportion of participants with PSA levels >or=2.0 and 4.0 ng/ml did not increase, but the biopsy compliance rate did increase, from 36% during 1997–1998 to 70% during 2005–2006.57
In 2016, there were 1,745 deaths from prostate cancer, accounting for 3.6% of all cancer deaths in men, with a crude mortality rate of 6.8 per 100,000 persons.3 The age-standardized mortality of prostate cancer increased, with EPACs of 16.7% and 0.7% during 1999–2002 and 2002–2014, respectively.22
The 5-year net survival rates of prostate cancer were 76.0% (95% CI 74.6–77.5%) and 89.9% (95% CI 89.2–90.5%) during 2000–2004 and 2010–2014, respectively.25 According to some studies, Korean prostate cancer patients have a higher risk for malignant characteristics, including higher Gleason scores, pre-operative PSA levels, and increased prostate volume, and are at more advanced clinical stages than are Western patients.5859
9. Pancreatic cancer
Pancreatic cancer constitutes the eighth most common cancer and the fifth leading cause of cancer-related death in Korea. In 2015, there were 6,342 (3,359 men and 2,983 women) cases of pancreatic cancer, accounting for 3.0% of all incident cancer, with a CR of 12.4 (13.2 in men and 11.7 in women) and an ASR of 7.0 (8.5 in men and 5.7 in women) per 100,000 persons. During 1999–2015, the incidence of pancreatic cancer was stable or slightly increased, from an ASR of 5.6 in 1999 to one of 7.0 in 2015 and an EAPC of 1.4%.2
In contrast to most other common cancers but consistent with the global trend for this particular type of cancer, mortality from pancreatic cancer has not decreased.60 The age-standardized mortality per 100,000 cases of pancreatic cancer slightly increased, from 5.4 in 1999 to 5.7 in 2015, with an EAPC of 0.3%. In 2016, there were a total of 5,614 deaths (2,901 men and 2,713 women) from pancreatic cancer, accounting for 7.0% of all cancer-related deaths in Korea.3
The 5-year net survival rate of pancreatic cancer increased from 7.6% (95% CI 7.2–8.1%) in 2000–2004 to 8.4% (95% CI 8.0–8.9%) in 2005–2009 and to 10.5% (95% CI 10.0–10.9%) in 2010–2014.25
Tobacco smoking is the major recognized risk factor for pancreatic cancer, and the estimated relative risk (RR) of pancreatic cancer was 1.5 (95% CI 1.3–1.7) in current smokers. Smoking-attributable cases were estimated to account for 15.5% (27.4% in men and 0.8% in women) of all pancreatic cancers and 14.9% (26.8% in men and 0.4% in women) of all deaths from pancreatic cancer.43 Being overweight or obese, diabetes, pancreatitis, and heavy alcohol consumption have also been related to the risk of pancreatic cancer incidence and mortality.61
10. Gallbladder cancer
Gallbladder cancer (GBC) is the ninth most common cancer, with 6,251 new cases (3,220 men and 3,031 women) accounting for 2.9% of all incident cancer in Korea in 2015.2 The CR and ASR per 100,000 persons were 12.3 (12.6 in men and 11.9 in women) and 6.6 (8.0 in men and 5.5 in women), respectively (Table 2). No significant sex difference was observed, with a female-to-male incidence ratio (F/M ratio) of 0.96 during 1999–2013. The most common histologic type of GBC was adenocarcinoma, which increased significantly from 1999–2003 to 2009–2013, with an ASR of 1.12–1.66 in men and of 1.11–1.45 in women.62 Recently, the incidence of gallbladder cancer decreased slightly, with an EAPC of −0.3% during 2004–2015.2 In most countries, the incidence in women is higher than that in men. The F/M ratio for the incidence of GBC was approximately 1.1 worldwide and in Asian countries, and it was 1.4 in European populations. In Korea, the incidence of GBC was higher in men, with an F/M ratio of 0.69 in 2012, which is similar to the 0.64 ratio in Japan.16
In total, 4,408 deaths from GBC (2,248 men and 2,160 women) were reported in 2016, accounting for 5.5% of all cancer-related deaths.3 Mortality from GBC decreased recently, from 5.2 per 10,000 persons in 1999 to 4.2 per 10,000 persons in 2015. During 2001–2015, a significant reduction in mortality from GBC was found in both sexes, with EAPCs of −2.8% and −2.6% in men and women, respectively (Table 3).2
The 5-year RSR of gallbladder cancer increased from 17.3% in 1993–1995 to 29.1% in 2011–2015, with an EAPC of 11.8% during this period. In 2011–2015, the 5-year RSR in men (30.2%) was slightly higher than that in women (28.0%).22
11. Non-Hodgkin lymphoma
Non-Hodgkin lymphoma (NHL) was the eleventh most common cancer in 2015, with a total of 4,396 (2,519 men and 1,877 women) cases. The CR and ASR per 100,000 were 8.6 (9.9 in men and 7.4 in women) and 5.9 (7.2 in men and 4.6 in women), respectively (Table 1). The incidence of NHL increased from 4.3 in 1999 to 5.9 in 2015, with a significant EAPC of 2.3% (Table 2). NHL was the eighth most common cause of cancer-related deaths in 2015, with a total of 1,771 deaths (1,026 men and 745 women) reported. The crude and age-standardized mortality figures were 3.5 (4.0 in men and 2.9 in women) and 2.8 (2.7 in men and 1.4 in women), respectively.2 In 2016, 1,778 deaths from NHL were reported, accounting for 2.2% of all-cause cancer deaths.3 However, the age-standardized mortality decreased from 2.1 in 1999 to 2.0 in 2015, with a significant EAPC of −0.5% during this period. The 5-year RSR also increased during these decades, as the 5-year RSR of 46.6% in 1993–1995 increased to 62.9% in 2011–2015, with an EAPC of 16.3%.2
CONCLUSION
During the past several decades, there have been noticeable, increasing trends in the incidences of thyroid and breast cancer in women, and of colorectal and prostate cancer in men. Despite these inclines of the past, recent trends clearly indicate a declination in the incidence of cancerous rates, and the incidence of stomach, liver, and cervical cancer in women has continually decreased since 1999. The number of cancer deaths increased by a factor of 2.7 from 1983 to 2016, and the age-standardized mortality has been decreasing by 3% every year. The 5-year RSR also improved during these decades, especially for stomach, prostate, and breast cancer, with 5-year RSRs of more than 90%.




 XML Download
XML Download