

 PDF
PDF ePub
ePub Citation
Citation Print
Print



서론
대상 및 방법
2005년 2월부터 2013년 5월까지 계명대학교 동산의료원에서 선천성 만곡족으로 진단 받고 Ponseti 방법12)으로 교정 치료한 환자 중 2년 이상 추적 관찰이 가능하였던 65명(102족)의 환자를 대상으로 하였다. 37명은 양측성 만곡족을 보였고, 28명은 일측성 만곡족을 보였다. 1) Ponseti 방법 후 1주 이내에 수술적 치료를 받은 환자, 2) 2년 미만의 추시 관찰기간을 가지거나 추시 소실된 환자, 3) 선천성 만곡족 이외의 선천성 증후군 및 신경근육 이상을 보이는 환자는 연구 대상에서 제외하였다. 모든 환자에서 비수술적 방법인 Ponseti 방법12)을 이용한 석고붕대 교정방법으로 치료를 시작하였으며, 모든 술기는 소아 정형외과 경력이 20년 이상 되는 제1저자에 의하여 시행되었다. 본 연구는 계명대학교 동산의료원 e-IRB에서 승인 받아 진행되었다(IRB No. 2016-05-011-005).
Ponseti 방법12)은 전족부를 회외전시킨 후 제1 중족골두를 밀어 올리면서 요족을 교정하고자 하였고 족근동의 거골 경부측에 손가락을 대어 반대로 압력을 가하면서 전족부를 외전시켜 전족부 내전을 교정하였다. 이때 종골-입방골 관절 경첩이 되지 않도록 주의하면서 장하지 석고붕대 고정술을 시행하였다. 석고 고정은 1주일 간격으로 교체하였고 4–6회 시행 후 교정이 만족스럽게 이루어져 족배 굴곡이 20도 이상 가능한 환아에서 외전족배 보조기 착용을 시작하였으며 족배 굴곡이 20도 이하이거나 첨족 변형이 남아 있는 환아 39명(63족)에서는 국소마취하에 아킬레스건 절단술을 시행하여 족관절을 20도 족배 굴곡시키고 70도 외회전시킨 상태로 2주간 장하지 석고붕대 고정술을 시행하였다.
Ponseti 교정방법의 초기 성패는 추가적인 수술 여부로 결정하였으며 수술 시행 여부로 두 군(A군: 초기 치료가 성공하여 수술을 시행하지 않은 군, B군: 재발 혹은 잔존 변형으로 인하여 수술을 시행한 군)으로 나누었다. Ponseti 방법에 의해 초기 치료가 완료된 상태에서 결과가 만족스럽지 못하거나 결과가 만족스러워도 추시 기간 중 재발한 환아의 경우 수술적 치료를 시행하였다. 수술적 치료는 평균 생후 24개월(8–56개월)에 시행하였다. 초기 치료 후 결과가 만족스럽지 못하거나 추시 기간 중 재발한 환아, 경골 염전이 동반되어 있으며 내족지 보행이 있는 환아의 경우 추가적으로 수술적 치료를 시행하였다.
모든 대상 환아에 대하여 전후면 족부 및 최대 족배 굴곡 상태에서 족관절을 포함하는 측면 족부 단순 방사선 촬영을 시행하였다. 전후면 족부 방사선 촬영은 정형외과 의사가 환아의 발을 잡은 상태에서 X선 방사 각도가 발등에 수직이 될 수 있게 하여 촬영하였고, 측면 족부 방사선 사진은 정형외과 의사가 블록을 이용하여 환아의 발바닥 전체를 접촉시킨 상태에서 최대 족배 굴곡을 시킨 상태에서 촬영하였다. 두 군의 방사선적인 족부 변형 상태 비교는 전후면 거종간 각(talo-calcaneal angle on anteroposterior view, TCA), 측면 거종간 각(talo-calcaneal angle on lateral view, LTCA), TCA 및 LTCA의 합(sum of TCA and LTCA, TCA anteroposterior+laterior [AP+Lat]), 전후면 거골-제1중족골간 각(talo-1st metatarsal angle on anteroposterior view, TFMA), 측면 경종간 각(tibio-calcaneal angle on lateral view at ankle full-dorsiflexion state, TicalA)을 지표로 정하여 측정하였다(Fig. 1). 모든 기준선은 해당 뼈의 장축을 기준으로 선을 그렸고 그 사이의 각을 측정하여 각 도를 기록하였다. 각 방사선 사진은 관찰자 내 신뢰도를 평가하기 위해 한 정형외과 의사가 2회씩 검토한 후 평균을 분석하였으며, 관찰자 간 신뢰도를 평가하기 위해 난수표를 통해 20족을 선정하여 각도를 측정하여 급내 상관 변수(intra-class correlation)를 통하여 분석하였다.
두 그룹 간의 초기 족부 변형 상태를 비교하고자 최초 방문 시 각 방사선적 지표를 측정하여 통계적으로 비교하였다. Ponseti 방법을 시행 후 족부 변형의 호전 정도의 차이를 확인하기 위해 A군에서는 최초 방문 시와 Ponseti 방법으로 치료 후 최종 추시 시 방사선적 지표들을 측정하였으며 B군에서는 최초 방문 시와 수술적 치료 직전, 최종 추시 시의 방사선적 지표들을 측정하여 각 시기별로 호전 정도를 평가하였다.
모든 결과는 IBM SPSS package ver. 21.0.1 (IBM Co., Armonk, NY, USA)을 이용하여 분석하였다. 정규성 가정을 만족하는 항목에 대해서는 paired t-test를 시행하였고, 정규성 가정을 만족하지 못하는 항목에 대해서는 Mann-Whitney 및 chi square 검사, Wilcoxon 부호순위 검정을 시행하였다. 95%의 신뢰 구간을 기준으로 분석하였으며, p-value 0.05 미만에서 통계적 의의를 지닌다고 해석하였다.
결과
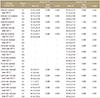
Ponseti 방법으로 치료를 시작할 당시의 환아들의 평균 연령은 생후 1.63주(A군: 1.45주, B군: 2.07주)였고, 최종 추시 시의 평균 연령은 6.67세(A군: 6.16세, B군: 7.86세)였다. 환자들의 추시 기간은 평균 3.95년(2.0-8.3년)이었다. 73족(71.6%: A군)에서 Ponseti 방법으로 치료 후 추가적인 수술 없이 성공적인 결과를 얻었고, 29족(28.4%: B군)에서 Ponseti 방법으로 치료 후 결과가 만족스럽지 못하여 추가적인 수술을 요하였다. 재발하는 족부 변형에 대하여 pie-crusting 술식을 이용한 경골-종골간 연장술(tibio-calcaneal lengthening) 9예, 입방골 설상 절골술을 포함한 거골-주상골 관절 유리술(tibio-navicular release+cuboid wedge osteotomy) 2예, 후경골근 유리술과 입방골 설상 절골술을 포함 혹은 포함하지 않은 거골-주상골 관절 유리술(posterior tibialis release+tibionavicular release±cuboid wedge osteotomy) 14예를 시행하였으며, Ponseti 교정에도 불구하고 잔존하는 족부 변형에 대하여 중족골 교정 절골술(metatarsal corrective osteotomy) 1예 및 경골 회전 절골술(tibia derotational osteotomy) 3예를 시행하였다. 추가적인 수술은 평균 나이 25.8개월(3–64개월)에 시행하였다. 추후 18족(17.6%)에 대해서는 추가적 2차 수술을 시행하였다(Table 1). Ponseti 치료 시 아킬레스건 절단술은 63족(61.8%)에서 시행하였고, A군에서 39족(53.4%), B군에서 24족(82.8%)에서 시행하였고, 아킬레스건 시행 여부에 따른 통계적 유의한 차이는 없었다.
두 명의 정형외과 의사가 무작위로 선택한 20족의 방사선 사진을 통해 각각 각도를 측정하여 관찰자 간 신뢰도를 평가하였으며, 신뢰성 점수는 모든 각도에서 85% 이상이었다. 모든 각도는 한 명의 정형외과 의사가 두 차례에 걸쳐 검토하였으며, 관찰자 내 신뢰도 점수는 모든 각도에서 95% 이상이었다. 치료 전후 및 초기 변형 각도를 평가하기 위해 각 측정값의 평균값을 구하여 통계적 분석을 시행하였다(Table 2, 3).
초기 방사선 소견상 LTCA 및 TicalA에서 두 군 간에 의미 있는 차이가 있었다. LTCA는 A군에서 33.99°±15.24°, B군에서 24.78°±15.25°, TicalA는 A군에서 79.03°±28.72°, B군에서 94.83°±24.13°로 초기 변형이 심할수록 수술 비율이 높게 나타났다(p=0.007, 0.010)(Table 4).
A군에서 평균 13.93주간 Ponseti 방법으로 치료 후 TCA가 평균 7.31°, TCA와 TCA의 합(TCA AP+Lat)이 평균 9.59°, TFMA가 평균 21.12°, TicalA이 평균 15.75°만큼의 호전(p=0.000)을 보였으며, LTCA에서는 통계적으로 의미 있는 변화가 없었다(p=0.179).
B군에서 평균 22.17주간 Ponseti 방법으로 치료 후 TFMA가 평균 11.77°만큼 호전(p=0.014)을 보였으며, TicalA이 평균 12.71°만큼의 호전(p=0.012)을 보였다. 그 외 방사선적 지표에서는 통계적으로 의미 있는 변화가 없었다(TCA, p=0.770; LTCA, p=0.973; TCA AP+Lat, p=0.865). TFMA, TicalA은 A군과 B군 모두에서 초기 평가와 비교하였을 때, 최종 추시상 의미 있는 호전이 있었다(Table 5).
고찰
지금까지 유·소아의 족부 변형에 있어서 단순 방사선 사진을 이용한 방사선적 측정을 통한 평가는 완전히 신뢰하기는 어려운 것으로 회자되어 왔다.13141516) Simons17)는 1978년 유·소아에서는 단순 방사선 사진상 골화 중심이 없거나 매우 작아서 선천성 만곡족의 평가에 있어서 방사선적 측정을 사용하는 것은 논란의 여지가 있을 수 있다고 기술하였다. 하지만 동시에 유·소아의 족부 위치의 오류로 인한 각도의 변화량은 매우 미미하다고도 기술하고 있다.
방사선적 평가의 질을 높이기 위해서는 첫째, 단순 방사선 사진 촬영 시의 올바른 발의 위치와 모양이 중요하며 둘째, 골화 중심의 축을 해부학적인 축과 최대한 일치하게 하여 오차를 줄이는 데 있다. 특히 후자의 경우 대상 환아의 나이가 어릴수록 골화 중심이 둥글기 때문에 각도를 잴 때 더 큰 오차가 생길 수 있으므로 주의해야 한다. 실제로 본 연구에서는 A군과 B군의 초기 방사선적 지표를 비교 분석했고 A군과 B군에서 각각 Ponseti cast를 통한 초기 치료 결과에 대해 분석했으며 B군에서는 초기 치료 후 술적 치료까지 마친 후의 치료 결과도 분석하였다. 본 연구의 결과에 따르면 LTCA 및 TicalA가 수술적 치료의 필요성을 예측할 수 있는 중요한 지표가 될 수 있을 것이다.
또한 TFMA, TicalA는 선천성 만곡족의 치료 후 치료 효과를 평가하는 데 있어 유용한 것으로 평가되었다. 이에서 종골과 거골이 모두 재태 26주경에 골화 중심 형성을 시작하나 종골의 경우 거골에 비해 장축의 형성이 빠르기 때문에1819) 경골과 종골의 장축을 비교하는 경종간 각 및 제1중족골의 장축을 측정하는 데 오차가 제일 적었을 것임을 짐작할 수 있다
본 연구의 제한점으로는 첫째, 본 연구는 후향적으로 이루어진 연구이며 두 그룹 간 치료 전 초기 족부 변형상태를 Diméglio score20) 등을 통하여 임상적으로 평가하지 못하여 방사선적 족부 상태의 평가와 임상적인 환아의 족부 상태의 평가가 실제로 연관성을 가지는지 확인하지 못하였다는 점이다. 둘째, 많은 연구에서 보조기 착용 순응도가 예후에 큰 영향을 끼친다는 보고21)가 있었음에도 불구하고 보조기 착용 순응도를 나타내는 객관적인 기준이 모호22)하여 본 연구에 포함하지 못하였다. 마지막으로 측정각들의 표준 편차가 커서 임상적으로 수술적 치료 여부를 결정하는 데 적용할 수 있는 기준치를 정하지 못하였다. 이들 제한점은 추후 환자군에 대한 지속적인 추시 및 추가적인 환자군의 포함을 통하여 파악할 수 있을 것으로 생각한다.





 XML Download
XML Download