

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Although ischemia in the distal areas of the limbs due to vascular occlusion is a well recognized systemic condition in patients who have diabetes, infarction of skeletal muscle, not associated with gangrene, is exceedingly rare and the paucity of published cases focused on this condition makes it difficult to determine the most appropriate methods of diagnosis and treatment. The authors encountered a case of diabetic muscle infarction with exquisitely tender swelling on the anteromedial aspect of thigh and herein report the diagnostic work-up and treatment performed on the patient.
Figures and Tables

Figure 2
Doppler ultrasonography shows normal vessel lumen and normal flow of the common femoral vessel.
Figure 3
Axial post-contrast computed tomography scan of the left thigh shows enlargement and low attenuation in the adductor and vastus medialis muscles with peripheral irregular enhancement (white arrows) and central enhancing foci. Note well fixed ring enhancement (black arrows) surrounding vastus intermedius muscle. There are many strands in the subcutaneous fat indicative of edema.
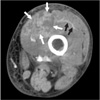
Figure 4
Axial fat-suppression T2-weighted fast spin echo (A) and coronal short tau inversion recovery (B) magnetic resonance (MR) images show enlargement and high signal intensity in the left thigh muscles, including adductors (asterisks), vastus medialis, sartorius and gluteus maximus. More superficially there is subfascial fluid. Diffuse subcutaneous edema at both sides is also noted. On coronal T1-weighted spin echo MR image (C), the affected muscles are slightly hypointense.


References
1. Angervall L, Steiner B. Tumoriform focal muscular degeneration in two diabetic patients. Diabetalogia. 1965. 1:39–42.

2. Aboulafia AJ, Monson DK, Kennon RE. Clinical and radiological aspects of idiopathic diabetic muscle infarction. Rational approach to diagnosis and treatment. J Bone Joint Surg Br. 1999. 81:323–326.
3. Chester CS, Banker BQ. Focal infarction of muscle in diabetics. Diabetes Care. 1986. 9:623–630.
4. Damron TA, Levinsohn EM, McQuail TM, Cohen H, Stadnick M, Rooney M. Idiopathic necrosis of skeletal muscle in patients who have diabetes. Report of four cases and review of the literature. J Bone Joint Surg Am. 1998. 80:262–267.
5. Lauro GR, Kissel JT, Simon SR. Idiopathic muscular infarction in a diabetic patient. Report of a case. J Bone Joint Surg Am. 1991. 73:301–304.
6. Hinton A, Heinrich SD, Craver R. Idiopathic diabetic muscular infarction: the role of ultrasound, CT, MRI, and biopsy. Orthopedics. 1993. 16:623–625.
7. Morcuende JA, Dobbs MB, Crawford H, Buckwalter JA. Diabetic muscle infarction. Iowa Orthop J. 2000. 20:65–74.
8. Umpierrez GE, Stiles RG, Kleinbart J, Krendel DA, Watts NB. Diabetic muscle infarction. Am J Med. 1996. 101:245–250.
9. Pope TL, Bloem HL, Beltran J, Morrison WB, Wilson DJ. Imaging of the musculoskeletal system. 2008. 1st ed. Philadelphia: Saunders;1035.
10. Delaney-Sathy LO, Fessell DP, Jacobson JA, Hayes CW. Sonography of diabetic muscle infarction with MR imaging, CT, and pathologic correlation. AJR Am J Roentgenol. 2000. 174:165–169.
 XML Download
XML Download