

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intramedullary nailing was introduced in the treatment of femoral shaft fractures resulting in excellent union19). Interlocking nailing provides more rotational stability for fixation of the fracture. Closed intramedullary nailing is a recent treatment for femoral shaft fractures2,17).
Less than 1% of cases of nonunion of femoral shaft fractures are treated with interlocking nailing16). However, the nonunion presented recently might be more tenacious than those previously reported. The causes of nonunion of femoral shaft fracture are based on many factors. There are several surgical options for treating femoral shaft nonunion after interlocking nailing: nail exchange, dynamization, and bone grafting and plate augmentation. Nail exchange was reported to be the best treatment for nonunion of femoral shaft fractures7,14) but the entire nonunion could not treated with only exchange nailing.
We introduced plate augmentation and bone grafting for the treatment of femoral shaft nonunion, leaving the interlocking intramedullary nail in situ to remove the rotational instability of the nonunion site. The remaining intramedullary nail could allow early weight-bearing rehabilitation after plate augmentation. Bone grafting performed simultaneously filled the bony defect and stimulated healing. This study evaluated the efficacy of various surgical options for treating femoral shaft nonunion after interlocking nailing.
MATERIALS AND METHODS
From January 1996 to December 2000, 31 cases of femoral shaft nonunion after interlocking intramedullary nailing were treated at our hospital and followed up for at least one year. Twenty-six subjects were male and 5 were female with a mean age of 38 years old. Twenty-five cases were due to car accidents and 6 were due to falls from a height. Twenty-three had closed fractures and 8 had open ones. The fractures were located at the middle 1/3 in 17 cases and at the distal 1/3 in 14. According to the Winquist-Hansen classification, there were 9, 5, 12 and 5 types I, II, III and IV fractures, respectively. The fractures were treated using three different types of reamed nails and one unreamed nail. Reamed nails were used for 26 fractures and unreamed nails were used for 5. Twenty-three fractures were fixed in a astatic mode and 8 were fixed in dynamic mode (Table 1).
The mean time between fixation of the fracture and the treatment for nonunion was 14 months (6-46 months). According to theWeber and Brunner classification, 26 showed oligotrophic nonunion and 5 showed hypertrophic nonunion.
The surgical options used for nonunion included dynamization, bone grafting, exchange nailing and augmentative plating with bone grafting. Exchange nailing was performed with a nail at least 2 mm larger in diameter than the previous nail. The nail was fixed in static mode. Partial weight bearing was allowed immediately after exchange nailing. For augmentative plating, plates with 6 or 8 holes were fixed across the nonunion site without removing the interlocking nail. If intramedullary nailing was not fixed in static mode, the intramedullary nail was changed to a dynamic mode before augmentative plating. The nonunion site was exposed through the posterolateral approach and checked for any motion at the nonunion site, particularly rotational instability. More than 3 cortices purchase in each side was sufficient to eliminate the motion. The nonunion site was filled with an autogenous bone graft that had beenobtained from iliac crest. The patient was allowed partial weight bearing with two crutches immediately after surgery.
Union was defined as an absence of pain and tenderness despite full-weight bearing with a disappearance of the fracture line through callus bridging in four cortices.
RESULTS
Twenty-eight of the 31 cases achieved union at the last follow-up. Three patients refused to undergo further surgery after the failure of the previous operation for nonunion. There were an average of 1.5 operations for every nonunion case. Radiological bone union required an average of 20 months (10-54 months) from the first operation to treat the femoral shaft fracture. One operation was sufficient to achieve union in 18 nonunion cases (58%). However, 11 patients required further surgery for nonunion. Three patients had three separate operations to achieve union.
Dynamization was used for 4 nonunion cases but all failed to achieve union. Of the 14 cases treated with bone grafting (12 in the first procedure and 2 in the 2nd), seven cases (50%) achieved union. Seven out of 13 cases (10 cases in the 1st procedure and 3 in the 2nd) (53%) treated with exchange nailing achieved union. Three of the six cases that did not achieve union were treated with a plate augmentation and bone grafting and achieved union but three cases refused further surgery to achieve union. All 14 cases (100%) treated with augmentative plating and bone grafting (6, 5 and 3 in the 1st, 2nd and 3rd procedure, respectively) achieved union.
DISCUSSION
Dynamization was not found to be beneficial for achieving union, particularly in comminuted fractures. It produced a significant instability at the nonunion site and femoral shortening. It is believed it is more important to prevent distraction and enhance the contact of the fracture site when fixing a femoral shaft fracture. Femoral shaft nonunion is no longer treated with dynamization.
In this study, bone grafting only in the treatment of the nonunion achieved union in only 50% of cases. However, bone grafting with an additional procedure tended to stimulate fracture healing. Bone grafting was performed at the time of augmentative plating in 14 patients and achieved union in all patients.
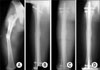
Most of the femoral shaft nonunion cases were treated successfully with exchange nailing using the next larger nail7,14). Exchange nailing is known to be the treatment of choice for femoral shaft nonunion (Fig. 1). Exchange nailing using a nail with a slotted compression hole can eliminate the fracture distraction and enhance the fracture stability in the treatment of femoral shaft nonunion with a short oblique or transverse fracture. Exchange nailing allows early weight bearing with low morbidity. However, all femoral shaft nonunions for which intramedullary nailing has failed were not considered appropriate for exchange nailing5). The rate of union rate ranged from 53% to 78% after the first exchange intramedullary nailing and 87% to 95% after the second procedure. In our study, 7 out of the 13 cases treated with exchange nailing achieved union, which is an unsatisfactory success rate. There are questions regarding exchange nailing for femoral shaft nonunion9,15). According to the study reported by Johnston9), the rotational stability of the interlocking intramedullary nailing was 3% of that of the normal femur. Rotation of 10-15° occurred at the fracture site without resistance in the femur with intramedullary fixation. This means that there was some limitation in the rotational stability of the interlocking intramedullary fixation. It was not difficult to notice the rotational movement at the nonunion site during augmentative plating even though the fracture had been fixed with static interlocking nailing. In the distal 1/3 femoral shaft fracture or comminuted fracture, exchange nailing with a larger diameter nail than that of the previous nail could not eliminate the rotational instability completely10). Nonunion following comminuted fractures do not appear to respond to exchange nailing as favorably as nonunion occurring after simple transverse or oblique fractures2,11). Four out of 6 failures with exchange nailing were the distal 1/3 and type III comminuted fracture. Exchange nailing cannot be recommended for distal femoral nonunion5). In the abovementioned cases, plate fixation with autogenous bone graft was a good surgical option. However plate augmentation and bone grafting without removing the intramedullary nail had more advantages such as a short operation time, less invasiveness and early weight bearing after surgery than plate fixation after removing the nail.
There are three surgical options for the treatment of nonunion after exchange nailing; repeated nailing, bone grafting and repeated nailing with bone grafting. However, we did not attempt secondary exchange nailing. Three of the 6 nonunion cases were treated with augmentative plating and bone grafting that had not achieved union after exchange nailing (Fig. 2). In our opinion, augmentative plating and bone grafting are better choices than repeated nailing. Although sufficient vascular supply is very important, stable fixation is also essential for achieving fracture healing. Augmentative plate fixation might improve the rotational stability11,13). Fourteen cases of nonunion of the femoral shaft were treated with plate augmentation and union was achieved in all patients. Plate augmentation with autogenous bone grafting is a useful method for treating oligotrophic nonunion due to a comminuted fracture. It requires bone grafting for the bone defect and plate augmentation for instability. There was some concern that plate augmentation after intramedullary nailing might cause a disastrous event in the vascular supply of the femur but this did not occur. Cole6) examined the vascular supply of the femur after intramedullary nailing and showed the whole vascular supply of the femur had been restored within 2 weeks after nailing. Our cases were treated with plate augmentation an average of 14 months after intramedullary nailing. Augmentative plating required limited exposure of 6 or 8 holes to fix the plate. Therefore, it might not destroy the vascularity of the femur. There was no serious problem and no secondary procedures were required for fracture healing after plate augmentation with bone grafting for nonunion regardless of whether there had been oligotrophic or hypertrophic nonunion. All nonunion cases that failed to be healed properly by other surgical procedures could be healed using plate augmentation and bone grafting.
CONCLUSION
Exchange nailing is not appropriate for all cases of femoral shaft nonunion and augmentative plating with bone graft was found to be a safe and useful method for treating femoral shaft nonunion after intramedullary nailing. Therefore, augmentative plating and bone grafting is the preferred treatment over repeated exchange nailing when union does not occur after exchange nailing for femoral shaft fracture.


 XML Download
XML Download