

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The first Winter Olympics was held in 1924 in Chamonix, France where Nordic skiing was the only skiing event.1) Snowboarding is a relatively new winter sport, and the current style of snowboarding device was first introduced in the late 1970s.2) Snowboarding was adopted for the Winter Olympics in 1998. Recently, snowboard cross, half pipe, etc. have become popular, and snowboarding has become an important part of winter sports. These sports have all been adopted for the Olympic Games.2) Ellison3) reported that of all skiing injuries, lower extremity injuries (42%) were twice as common as upper extremity injuries (24%). In contrast, injuries of the upper extremity account for approximately 50% of all snowboarding injuries and are nearly twice as prevalent as skiing injuries of the upper extremity.45) As the popular winter sport changes, the injured part of the body also changes. With the growing ratio of upper- to lower-extremity injuries during the alpine skiing and with the booming popularity of snowboarding, shoulder injuries have been seen with increasing frequency.
Previous studies reported on shoulder injury in skiing and snowboarding among the general public; those papers did not address injuries in elite athletes. In addition, to the best of our knowledge, there are no articles on analysis of shoulder injury in one large sports event. In this paper, we describe and analyze the shoulder injuries that occurred in elite athletes during the 2018 Winter Olympics in Pyeongchang.
METHODS
Over 2,833 athletes from 92 countries participated in the 2018 Winter Olympic Games. During the international sports event, 13 competition and 10 non-competition venue medical centers, two polyclinics, and two Olympic hospitals were operated.6) We reviewed the data of all Olympic athletes who visited venue medical centers, polyclinics, and Olympic-designated hospital during the Olympic Games (January 26 through February 28, 2018).
Definition of Shoulder Injury and Illness
We differentiated injury from illness in the patients with shoulder pain. We defined injury as the appearance of new symptoms and recurrence of symptoms after full recovery due to trauma during the Olympic Games.7) Therefore, athletes who participated in the games before complete rehabilitation of pre-existing conditions were not included in the study. Injuries included both direct trauma and overuse injuries. Overuse injury was defined as an injury that occurred during a game or training and was caused by repeated use without direct trauma. Illness was defined as the presence of symptoms that started without any trauma.
Data Collection
All medical records from venue medical centers and polyclinics were stored through electronic medical records (EMRs) during the Olympics. We collected Olympic EMR data and patient information obtained from Olympic medical service teams about athletes who complained of shoulder pain.
Basic information of each patient, such as athlete's accreditation number, age, nationality, date of birth, sport discipline/event, visiting date, injury time/place and vector, and game/training, was collected. Also, medical information such as injured body part, injury mechanism, diagnosis, and laboratory result was collected. And if the patient underwent a radiographic examination, we collected the images and readings from certified musculoskeletal radiologists. We used the athlete's accreditation number to control for duplicates. For duplicate cases, the most recent diagnosis was used for analysis.
We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Yonsei University Wonju College of Medicine (IRB No. CR318001). Informed consent was waived.
RESULTS
During the Olympics, a total of 14 athletes visited a clinic for shoulder-related symptoms (9% of total athlete injuries). Among them, 11 were men and three were women and their average age was 24.5 years (range, 17 to 32 years). Five athletes were injured in a game and nine were injured in training. In four patients, the injury was due to overuse; ten patients had direct trauma-related symptoms, one after being hit by an opponent and the other nine after a collision with the ground or an object. None of the patients complained of shoulder pain due to illness without trauma. In addition, all the injury-related symptoms newly developed, not recurred, after trauma. In three patients, shoulder symptoms were accompanied by other symptoms: back pain (n = 1), finger pain (n = 1), and posterior neck pain, shoulder pain, and knee pain (n = 1). The remaining patients had only shoulder pain.
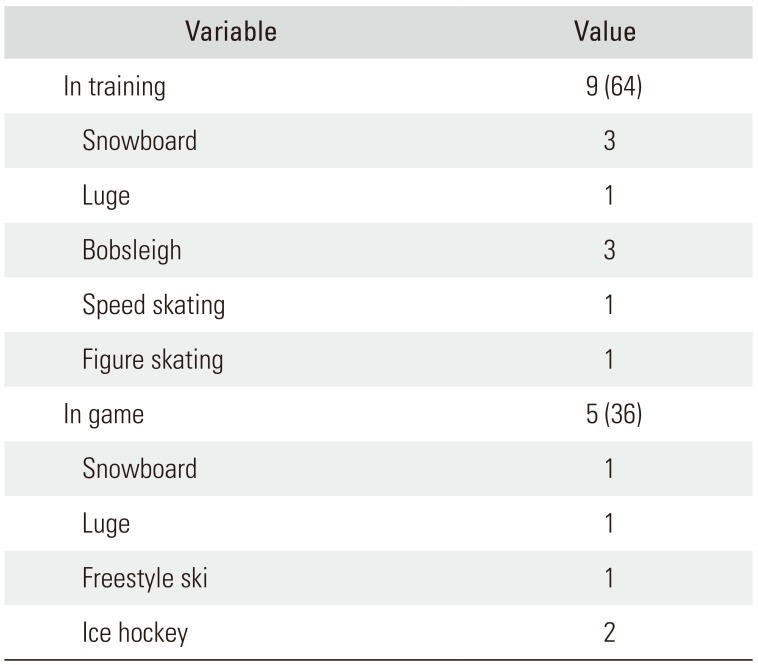
The most common cause of shoulder pain was snowboarding (one case in big air and three cases in slopestyle), followed by bobsleigh, luge, ice hockey, speed skating, figure skating, and freestyle ski (Table 1). The patients with shoulder pain underwent imaging tests according to their symptoms: radiography in six patients, computed tomography (CT) in three, ultrasound in three, and magnetic resonance imaging (MRI) in two.
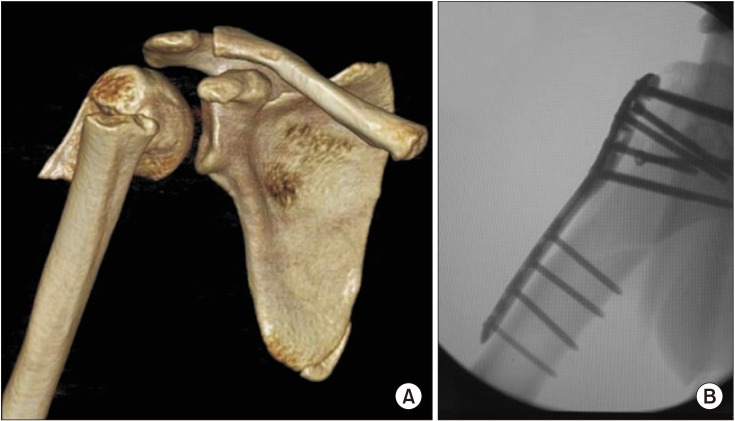
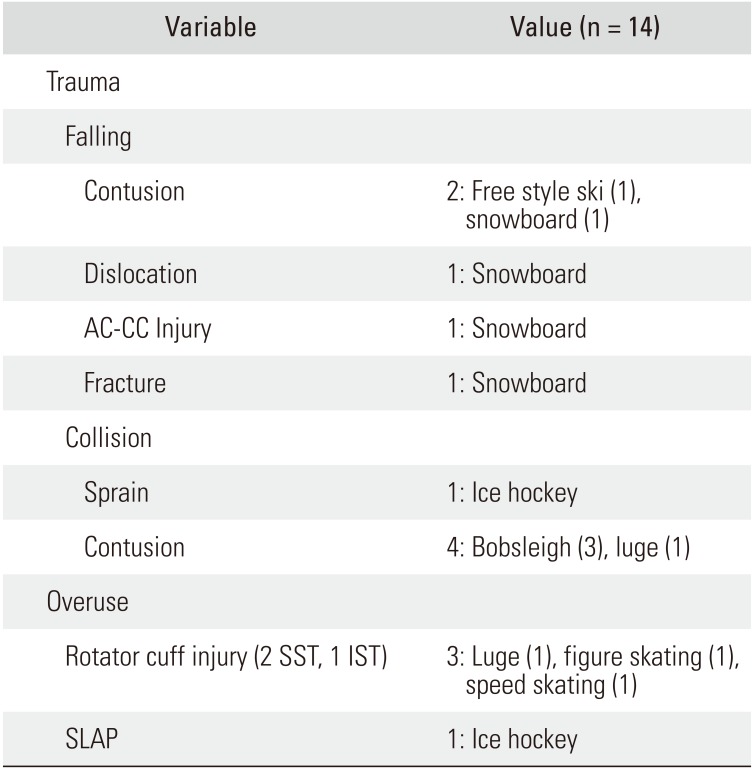
The most common diagnosis was contusion (n = 6), followed by rotator cuff injuries (n = 3), superior labrum from anterior to posterior (SLAP) lesion (n = 1), sprain (n = 1), acromioclavicular-coracoclavicular (AC-CC) injury (n = 1), dislocation (n = 1), and fracture (n = 1) (Table 2). The shoulder dislocation was accompanied by a Bankart lesion (Fig. 1).8) The fracture was accompanied by an injury to the surgical neck of the humerus and scapular body (Fig. 2). The SLAP lesion was diagnosed by MRI with physical examinations such as Speed test and Yergason's test; the dislocation with Bankart lesion was diagnosed by MRI and X-ray. All rotator cuff injuries where shoulder pain newly developed after trauma were diagnosed by ultrasound. The remaining conditions were diagnosed by X-ray. The AC-CC injury patient and one of the patients with contusion underwent CT to confirm that there was no fracture. The fractured patient underwent CT for preoperative planning.
Three patients required surgery: one patient with humerus fracture underwent surgery at the Olympic hospital and the others patients (shoulder dislocation with Bankart lesion or AC-CC injury) returned to their home country for surgery. Patients who did not need surgery were prescribed analgesics and underwent conservative management. Patients with AC-CC injury or shoulder dislocation were prescribed an orthosis and then returned to their home country for surgery.
DISCUSSION
There are large-scale studies of shoulder symptoms related to skiing and snowboarding in the general population.8) Sasaki et al.9) reported that the incidence of snowboarding injuries is three times higher than that of skiing injuries, shoulder is the most commonly injured site in the upper limb during skiing and the second most commonly injured site in the upper limb in snowboarding.
To the best of our knowledge, this study is the first epidemiologic study on shoulder injury conducted during a huge sports event involving a variety of competitions for elite athletes. The results showed the number of athletes with shoulder injuries was the highest in snowboarding. Since snowboarding became an official Olympic sport in 1998, other snowboarding disciplines, such as halfpipe, big air, and slopestyle, have been gradually added to the Olympic program. These types of sports require aerial acrobatics (large jumps with landing and falls from significant height) and thus carry an inherently higher risk of significant injury. By contrast, the incidence of shoulder injuries was unexpectedly low in ice hockey involving intense physical exertion; this may be attributable to a variety of powerful safety equipment for ice hockey and the availability of a team doctor who would handle simple bruises and contusions on the spot, obviating the need to use the Olympic medical service.
Shoulder injury due to trauma in winter sports is associated with a fall or collision.2) In this study, five of the traumas were caused by a fall and the remaining five occurred in a collision. There are two major mechanisms of injury of the shoulder associated with falling. One is an abduction-external rotation force against an outstretched arm by the slope during a fall (indirect injury). The other is direct loading on the shoulder (direct injury).21011) All except one in this study were direct injuries. This may be related to the effort to minimize damage by adjusting the posture of the arm when falling as an elite athlete.
In patients with nontraumatic pain in the shoulder, additional examinations revealed a SLAP lesion or rotator cuff injury related to repetitive motions rather than direct loading on the shoulder occurring in speed skating and luge. Repetitive motions may cause a minor trauma to the shoulder joint that will gradually lead to development of symptoms.12) There has been extensive research on the association of rotator cuff disease with overhead activity in baseball players and swimmers.13) However, there is a lack of research on the relationship between winter sports, such as speed skating and luge, and shoulder disease. In future studies, it will be necessary to investigate the relationship of winter sports with shoulder disease, not with trauma.
This study has the following limitations. First, presumably not all athletes with shoulder injury visited the venue medical centers, polyclinics, or Olympic-designated hospitals. Second, we may have missed some cases of injury that occurred in the early period of the Olympic Games. Until day 3, there were some errors in the EMR system, so the paper chart had to be transported to the EMR after outpatient clinics hours. For these reasons, the prevalence rate of shoulder injury may have been underestimated. Third, this study covered only one Winter Olympic Games; the number of cases may not be sufficient to draw definite conclusions.
The development of winter sports safety equipment contributed to the reduction in lower extremity injuries, whereas the diversification of winter sports events led to an increase in injury to the shoulder joint. Although there have been many studies on upper extremity injury in skiing and snowboarding, there have been no epidemiology studies of shoulder injury in elite athletes especially in the Winter Olympics with various sports events. If the risk factors of shoulder injury can be established by continuing research in the future, it will be helpful to prevent injury and devise safety measures for athletes.
In conclusion, of 2,925 athletes from 92 countries who participated in the PyeongChang Winter Olympic Games, 14 athletes visited the clinics for shoulder injury. Results of this epidemiological study can be useful for preventing common shoulder injury in athletes and preparing proper treatment and first aid for the next Winter Olympics.

 XML Download
XML Download