

 PDF
PDF ePub
ePub Citation
Citation Print
Print


While chair sitting is the most common position in modern daily life and work, in Asian countries, including Korea and Japan, flooring sitting is more common at home, such as kneel sitting in Japan and cross-legged sitting (tailor's position) in Korea. However, the impact of floor-sitting positions on the spinopelvic alignment was not studied previously in contrast to the extensive research on the sagittal lumbar and pelvic alignments in standing and chair sitting positions.1234)
According to Lord et al.,1) the angle of lumbar lordosis in standing was nearly 150% higher on average than that in sitting. The results indicated the benefit of using a sitting lumbar support for prevention of decreasing lumbar lordosis. It has been well known that the spinopelvic alignment in chair sitting position is different from that in standing position. However, the impact of the two floor-sitting positions (Korean and Japanese styles) on the spinopelvic alignment has not been studied yet. Therefore, we carried out this pilot study to elucidate the influence of the two sitting positions familiar in Asian culture on the lumbar spine and pelvis.
METHODS
Materials
Sixteen healthy volunteers (10 males aged 23–38 years and six females aged 20–25 years) with normal lumbar spine and hip joints and normal gait were the subjects of this pilot study. None had toe-in gait. All subjects signed the provided written informed consent document after explanation of the study protocol. This study was approved by Institutional Review Board of Cheju Halla Hospital.
Methods
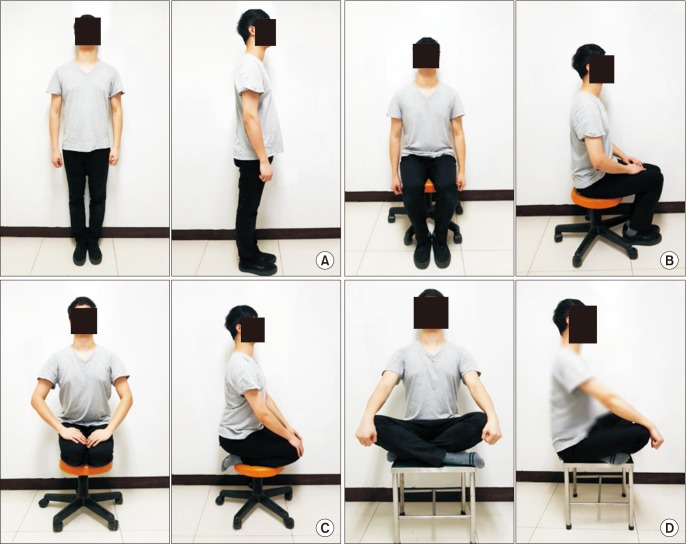
All subjects had the frontal and lateral radiographs of the whole spine including the hip joint taken in the standing, chair sitting, Japanese style kneel sitting, and Korean style cross-legged sitting positions with their hands placed over the laps (Fig. 1). For chair sitting, a height adjustable chair was used to accommodate each subject to sit with 90° flexed hips. In this study, deep hip and knee hyperflexed sitting (squatting) was not included. Care was taken to standardize each sitting position by pretest sitting position training. All subjects were asked to take comfortable upright position in sitting.
Radiography
All subjects repeatedly simulated the above-listed comfortable natural positions before radiography. Collimation was set superior to the cervical spine and inferior to the sacrum and both hips. Additionally, lateral radiographs of the lumbar spine and pelvis including both hips were taken.
Measurements of Each Parameters
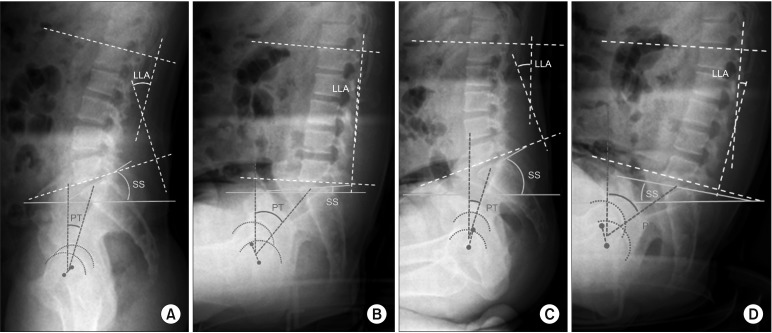
The following parameters were measured in each subject: (1) lumbar lordotic angle (LLA), the angle from the upper endplate of L1 to the upper endplate of L5; (2) sacral slope (SS), the angle between the sacral plate and a horizontal line; (3) pelvic tilt (PT), the angle between the line connecting the midpoint of the sacral plate to the axis of femoral heads and a vertical line; and (4) pelvic incidence (PI), the angle between the line perpendicular to the sacral plate at its midpoint and the line connecting the midpoint to the axis of femoral heads (Fig. 2).
RESULTS
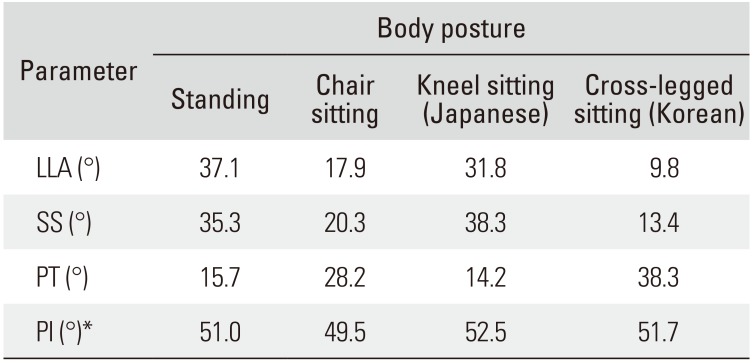
In the standing position of the 16 subjects, the average LLA, SS, PT, and PI were 37.1°, 35.3°, 15.7°, and 51.0°, respectively: the values were 35.1°, 33.7°, 15.4°, and 49.0°, respectively, in 10 males, while in six females, the values were 39.1°, 37.0°, 16.1°, and 53.1°, respectively. Between the two sexes, there was almost no noticeable difference.
In chair sitting of the 16 subjects, the average LLA, SS, PT, and PI were 17.9°, 20.3°, 28.2°, and 49.5°, respectively: the values were 13.8°, 16.5°, 27.5°, and 44.1°, respectively, in 10 males, while in six females, the values were 22.1°, 24.1°, 28.9°, and 54.9°, respectively. In females, LLA and SS were larger by 60% and 46%, respectively, than those in males.
In Japanese style kneel sitting, the average LLA, SS, PT, and PI in the 16 patients were 31.8°, 38.3°, 14.2°, and 52.5°, respectively: the values were 32.0°, 37.7°, 11.2°, and 49.0°, respectively, in 10 males and 31.6°, 38.9°, 17.2°, and 56.1°, respectively, in six females. Only PT was 54% larger in females than males.
In Korean style cross-legged sitting, the average LLA, SS, PT, and PI were 9.8°, 13.4°, 38.3°, and 51.7°, respectively: the values were 10.0°, 7.6°, 42.1°, and 49.8°, respectively, in 10 males and 9.6°, 19.2°, 34.5°, and 53.7°, respectively, in six females. All parameters except for LLA showed slightly larger values in females than in males.
LLA in standing (37.1°) and Japanese style kneel sitting (31.8°) were very similar. Remarkable reduction in LLA was observed in Korean style cross-legged sitting (9.8°). LLA in chair sitting (17.9°) was below half of that in standing (Table 1). SS in standing (35.3°) and Japanese style kneel sitting (38.3°) were similar. SS was remarkably reduced in cross-legged sitting (13.4°). PT was largest in cross-legged sitting (38.3°). PT values were similar in standing (15.7°) and kneel sitting (14.2°). PI values were similar in all positions.
DISCUSSION
There has been an increasing recognition of the importance of the sagittal plane contour of the spine for normal function of the spine in various positions. Among the sagittal spinal curves, lumbar lordosis plays a role in the maintenance of an efficient upright position. Studies have reported on the negative impact of reduced lumbar lordosis. There have been several previous studies on the sagittal lumbar and pelvic alignment in standing and chair sitting. 12345678) However, the sagittal lumbopelvic alignment in the sitting position on Tatami mats in Japan and Ondol floor (heated floor) in Korea have not been investigated.
Understanding the geometrical compromise is important in analyzing the anterior trunk imbalance and subpelvic compensation;910) the pelvis rotates on the bicoxofemoral axis, tilting anteriorly (“pelvic anteversion”) and posteriorly (“pelvic retroversion”) with the cranial point of the pelvic block tilting forward and backward. The extent of sacral tilt can be estimated from the angular variation in SS and PT. The limit of posterior PT available to compensate the anterior sagittal imbalance depends on the PI: the bigger the PI is, the bigger the availability for posterior PT. On the contrary, patients with small PI have lower potential for compensation. When compensatory tilt reaches the limit, the hip joints have no reserves for further extension and encounter a posterior block, at which point the patient will flex his or her knees.
In some patients, SS is small in the standing position (“posterior tilt”), and the sacrum shows vertical alignment on lateral views. In other patients, the sacrum is very horizontal in the standing position, with a slope of often over 50° (“anterior tilt”).
In general, the pelvis tilts backward during the transition to the sitting position. SS diminishes to 20° to 25° on average, sometimes as low as 5° to 10° or even below 0°. Depending on the height of the seat, individual pelvic morphology, and associated spinal pathology, a variable PT is observed with the more or less vertical sacrum. The difference of SS between the standing and the sitting positions corresponds with the flexion potential of the lumbosacral junction (available extrinsic pelvic flexion), which is distinct from potential hip joint flexion (accidental intrinsic pelvic flexion).6810)
The process of sitting down considerably alters the orientation of the anterior pelvic plane which is the reference for adjusting acetabular cups in total hip arthroplasty. It is well known that Far Eastern Asians (Japanese and Koreans) traditionally sit on the floor, though nowadays the younger generations live a more westernized lifestyle. However, even nowadays, a banquet venue offers two different kinds of seats for chair sitting and floor sitting on a cushion in these countries. Considering that banquets mostly last over 2 or 3 hours, sitting positions may affect the lower back structure (lumbar spine and pelvis) and can cause lower back pain. Thus, we set out to assess the impact of sitting positions in the current study among volunteer subjects without lower back and/or hip disorders.
Biomechanically, in the chair sitting position, the anterior lumbar column of the vertebra (i.e., disc) receives greater compressive stress at the lumbosacral junction, whereas in the standing position, the posterior column (i.e., facet joints) receives greater lordotic stress.
In case of the kneel sitting, both hips are flexed over 90° with some internal rotation, while in the cross-legged sitting, both hips are flexed nearly to 90° or over with external rotation. We conjectured that the hip position in different sitting positions may have remarkable influence on the spinopelvic parameters. To test our conjecture, we meticulously evaluated the impact of sitting positions on the lumbosacral spine and pelvis in this study.
In this study, LLA was similar in standing and kneel sitting, and remarkable reduction of LLA was observed in cross-legged sitting; SS was similar in standing and kneel sitting, and SS was remarkably reduced in cross-legged sitting; and PT was largest in cross-legged sitting and similar in standing and kneel sitting.
It is of note that the values of the parameters were remarkably similar in standing and kneel sitting, while the three parameters had noticeably different values in chair sitting and cross-legged sitting.
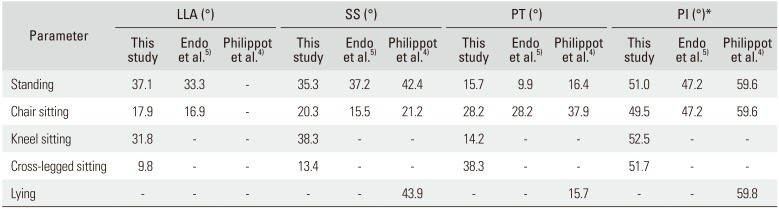
According to Endo et al.,5) compared to the standing position, LLA decreased by 50% and PT increased by 185% in sitting. In our study, LLA in standing was 37.1°, which was similar to that in the study by Endo et al. (33.3°).
In the current study, LLA was 31.8° in kneel sitting and 9.8° in cross-legged sitting; thus, it decreased by 26 % only in cross-legged sitting compared to that in standing. PT in kneel sitting (14.2°) was similar to that in standing (15.7°). But, in cross-legged sitting, PT increased by 244% (38.3°) of that in standing (15.7°). Based on these findings, it can be deduced that chair sitting and cross-legged sitting greatly affect LLA in comparison with standing and kneel sitting.
In the series of Philippot et al.,4) in the standing position, SS and PT were 42.4° and 16.4°, respectively (Table 2), while those in chair sitting were 21.2° and 37.9°, respectively (Table 3). Thus, in the Philippot et al.'s series, PT and SS, in particular, were a little larger than those in the current study and Endo et al.'s series. However, Endo et al. and Philippot et al. did not measure the values in two other sitting positions, though Philippot et al. included measurements for lying (Table 4). Philippot et al.4) admitted that in their series, PI was higher along with the average age of their study subjects, and they described that PI values were age-related. However, it is not sure whether PI could represent natural evolution with adaptation of PI to spine status, resulting in tipping of the pelvis toward the back and thus increasing tension of the hip-flexing muscles and hip flexion. Standing has been generally considered a working position compared to sitting, the resting position. Based on these concepts, it can be said that Japanese style kneel sitting is a type of working position, while Korean style cross-legged sitting is a less energy-consuming resting position. Chair sitting is the intermediate resting position.
The limitations of this study include the small number of subjects and lack of comparison with a large scale age- and sex-matched subjects. In an attempt to overcome this limitation, we have a further large scale study planned to elucidate unharmful sitting positions for all. Our results are consistent with those reported by the previous authors such as Roussouly et al.,8) Lee et al.,9) and Yang et al.10) They reported that the sagittal alignment of the human spine and pelvis in a standardized standing position was highly variable in different individuals, but they did not study the spinopelvic alignment in any type of sittings. In addition to confirming the results demonstrated in previous publications on spinopelvic parameters according to body postures, the study provided relatively new data related to the influence of two sitting positions, kneel sitting and crosslegged sitting, on the spinopelvic alignment.


 XML Download
XML Download