

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A rising number of trochanteric fractures associated with an increasingly elderly population have recently been reported.12) The key to a successful clinical outcome is early mobilization, allowing immediate full weight-bearing and rehabilitation.3) As stable fixation between the femoral head and femoral shaft is essential, a short intramedullary nail is the preferred choice, owing to its biomechanical and technical advantages,345) such as being less invasive and involving a shorter skin incision and less blood loss. Although intramedullary nailing has become popular for these reasons, some complications have been reported. Among these, two major complications-femoral shaft fractures and cut-out,67) which require revision surgery-are serious.
When this operation was in its infancy, a number of femoral shaft fractures were reported, especially in the USA; therefore, it was believed to be dangerous and not to be recommended. However, a modification of the technique developed in Asia and Europe, which removes the need for hammering and instruments and uses shorter and thinner nails, has decreased this complication dramatically.
However, cut-out is still a serious and unresolved complication. Previous reports have concluded that factors such as a screw positioning are the cause of this complication.8) However, in our observations, this can occur even when the screw is inserted at the optimal site. Fig. 1 shows our hypothesis that a "lack of bony support" is the most important factor involved in such complications, and we consider that the degree of sliding would be the indicator to evaluate the factor. However, orthopaedic surgeons cannot control lack of bony support because it is fixed at the point of injury and we have to accept the occurrence of excessive sliding to some extent. Therefore, we focused on the management of femoral head rotation to prevent cut-out in many cases. For this purpose, a blade has been developed to prevent femoral head fixation. There are two types of blade: a cylindrical spiral blade and a non-cylindrical H-shaped blade. The purpose of this study is to compare the capability of these three types of femoral head fixation devices with regard to the prevention of femoral head rotation. In this report, we use the term "femoral head fixation device" (HFD) as a general term to include both hip screws and various types of blades.
METHODS
Between July 2005 and December 2009, 216 patients with trochanteric or basal neck fractures, transferred to our institution's emergency department, met the present study's inclusion criteria. Of these, 206 aged over 60 years were enrolled in the study. The exclusion criteria were pathological fractures, fractures associated with polytrauma, fractures associated with previous surgery on the ipsilateral femur, intracapsular femoral neck fractures, and subtrochanteric fractures. The Institutional Review Board of Takatsuki General Hospital approved the study.
We used a gamma 3 nail (GMN, Stryker, Mahwah, NJ, USA) as the screw-type HFD in 66 cases, a gliding nail (GLN, Smith & Nephew, Memphis, TN, USA) as the non-cylindrical blade in 76 cases, and a proximal femoral nail antirotation (PFNA, Synthes, Oberdorf, Switzerland) as the cylindrical blade in 64 cases (Fig. 2). The selection of HFD changed during the study: from 2005 to 2008, we used GMN and GLN, but since 2008, we have used PFNA.
When using these three implants, we generally recognized their features as follows: the GMN was developed in an attempt to overcome several problems, such as the disadvantage of the dynamic hip screw and fracture of the base of the great trochanter when nailing with a Zickel nail. GMN transmits weight closer to the calcar than the dynamic hip screw and it has greater mechanical strength.9) PFNA is preferred because some surgeons believe that the helical blade design affords rotational and angular stability to the fracture. Another advantage of PFNA is that drilling of the femoral head is not required and it can preserve bone stocks by compressing the surrounding cancellous bone when inserted.1011) GLN also has a rotationally stable blade profile but differs in having an H-shaped blade.7) In biomechanical tests, GLN showed a reduction of 50% in the transmigration rate compared with GMN and 75% in comparison with the PFN double screw.712)
All surgeries were performed under fluoroscopic closed reduction. All surgeons were well trained and were supervised by an experienced surgeon (TH, MT, and MD) to confirm and guide the procedures. The intramedullary nail was inserted from the tip of the great trochanter after reaming the medullary canal up to the minor trochanter. The HFD was inserted using the respective target device aiming at the center of the femoral head in both anteroposterior and lateral views.
In our institution, all patients start rehabilitation as soon as practicable after surgery. For example, exercises such as standing at the bedside and partial and full weight-bearing were also allowed (as far as it could be tolerated) with the assistance of a physiotherapist shortly after surgery.
The fracture type (according to Jensen's classification), operating time, degree of sliding of the HFD at two weeks postoperatively, and the occurrence of femoral head rotation were evaluated and compared among the devices (evaluated by NC, TH, and TN). With regard to the follow-up time point, serious complications such as cut-out or femoral shaft fractures tend to be observed even during the early postoperative period.13) Therefore, we decided to evaluate the degree of sliding of HFD at two weeks postoperatively for the early detection of complications.
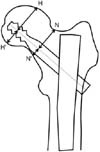
We measured the degree of sliding of HFD (Fig. 3). If we define the HFD axis as AB, and the intersection of AB and the nail axis as C, then the central length was calculated as AC / AB × actual HFD length; the degree of sliding was calculated by subtracting the central length at two weeks postoperatively from the length just after the surgery.1415) We also assessed femoral head rotation radiologically at two weeks or more postoperatively. Femoral head rotation was confirmed by an apparent change in H': H or N': N (Fig. 4). Postoperative follow-ups were planned at two weeks post-surgery, one month after discharge from hospital, followed by monthly until six months post-surgery, and thereafter according to the estimated occurrence of bone union.
Statistical analysis was performed using the SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). For statistical evaluation, we used the chi-test and one-way analysis of variance among the three groups, and the t-test among two groups. A p < 0.05 was considered significant.
RESULTS
A total of 41 male and 165 female subjects, with an average age of 84.7 ± 7.3 years (mean ± standard deviation; range, 60 to 98 years) were included in this study. No significant differences were found with regard to age and gender among fracture repair devices (p > 0.05). No enrolled patients were lost to follow-up or died before 6 months. Fracture repair devices and fracture types are shown in Table 1. GLN was used predominantly for basal neck and comminuted fractures, but the distribution of bone fracture type did not differ among the three groups (p > 0.05). Mean operating time and standard deviation were 31.5 ± 12.0 minutes, 34.8 ± 12.6 minutes, and 33.3 ± 11.7 minutes for GMN, GLN, and PFNA, respectively, with no significant differences among the three groups (p > 0.05). A comparison of the degree of sliding of GMN according to whether femoral head rotation was observed showed that this was significantly higher in cases with rotation (p < 0.05) (Table 2). The mean sliding length was measured and no significant differences were noted for mean degree of sliding among the three groups (p > 0.05) (Table 3). The frequency of fracture type leading to femoral head rotation among the three groups is shown in Table 4. Significant differences were found for the occurrence of femoral head rotation in PFNA (p < 0.05) but not in GMN (p > 0.05). Femoral head rotation was observed in 15 cases of GMN (22.7%), no case of GLN (0%), and 5 cases of PFNA (7.8%). Significant differences with respect to the occurrence of femoral head rotation were observed among the three groups (p < 0.05) (Table 5). Furthermore, significant differences were observed between GLN and PFNA (p < 0.05).
There were no intraoperative complications, but three patients suffered the postoperative complication of cut-out. In two patients (one GMN and one GLN), the cause of the cut-out was falling, as opposed to natural causes. These patients were managed by total hip replacements, and the results were satisfactory. In one patient with PFNA, perforation of the blade through the femoral head occurred following a fall on the buttocks three weeks postoperatively; bipolar hip hemiarthroplasty was performed, and the results were satisfactory. No collapse or periprosthetic fractures were observed during the follow-up periods.
DISCUSSION
Although it is generally believed that cut-out of HFD occurs after poor HFD positioning,8) it can also occur in patients where the HFD is in an acceptable position within the femoral head. We previously hypothesized that in GMN, the occurrence of cut-out was dependent on fracture type; in fractures with insufficient contact between bones, an excessive degree of sliding of the HFD could occur because of the lack of bony support, followed by femoral head rotation and subsequent cut-out. In contrast, with regard to the relationship between the increased sliding of the screw and cut-out, we found insufficient evidence of this in the literature.16) We consider that an excessive degree of sliding of the HFD might lead to insufficient fixation followed by cut-out because when we examined patients treated by GMN, we discovered an excessive degree of sliding and a high level of femoral head rotation. In contrast, no significant differences were observed when we examined the degree of sliding in GMN, GLN, and PFNA. It appeared that femoral head rotation occurred more frequently in comminuted fractures. As mentioned above, we consider that the degree of sliding was influenced more or less by the type of fracture; however, as this was a patient-dependent factor, it was outside the control of the orthopaedic surgeon. Therefore, we reconsidered that the reasons for the higher incidence of femoral head rotation observed in GMN compared with the other two HFDs was not due to the degree of sliding, but to differences in the rotational stability of the HFD. With respect to the relationship between femoral head rotation and cut-out, many authors have reported the importance of femoral head rotation as the cause of cut-out.171819202122) Taking our results into consideration, we also emphasized that femoral head rotation would lead to implant cut-out. Therefore, prevention of femoral head rotation can reduce the possibility of cut-out. From this viewpoint, the single screw-type HFD was at a disadvantage because it virtually had no ability to prevent rotation. Alternatively, the use of two screws was introduced to prevent rotation of the femoral head (PFN, Synthes). However, this technique proved to be less popular because it was a relatively complex procedure and involved the loss of bone stock and an unexpected screw movement called the Z-effect,2324) and higher revision rates using PFN were reported, e.g., a cut-out rate of up to 8%.625)
Blade-type HFD is another solution for preventing femoral head rotation.26) In this study, femoral head rotation was significantly less frequent in patients with blade-type HFDs than in those with single screw-type HFDs. Strauss et al.27) reported the biomechanical superiority of a blade compared with a hip screw, and several other published reports have shown that blade-type materials provided greater resistance to cut-out than lag screw design. 2028) In addition, blade-type HFDs have the further advantage of preserving cancellous bone because they are inserted in such a way to compress the surrounding cancellous bone without reaming and have a smaller cross-section and greater contact area.729)
We used two types of blades: one cylindrical (PFNA) and the other non-cylindrical (GLN). Gehr et al.7) reported zero occurrence of cranial perforations or cut-out when GLN was used. As GLN has an H-shaped cross section at the top, but is not constricted at the base, cancellous bone is compressed at this point and protected against perforation. In our study, GLN completely prevented femoral head rotation, whereas five cases were observed with the use of PFNA. In addition, we revealed that femoral head rotation occurred more frequently in comminuted fractures (according to Jensen's classification). From these results, we suggest that blade-type materials, particularly a non-cylindrical blade such as GLN should be used for such severe fracture types to avoid the likelihood of femoral head rotation leading to cut-out.
We consider that there are three limitations to the study. First, it is a retrospective study and the choice of the three implants used was not arbitrary, and the selection of the three implants was not randomized. Second, bone mineral density was not measured as a parameter of osteoporosis in all patients; we had to exclude the data on osteoporosis despite recognizing this as an important factor in cut-out. Third, with regard to measurement of the degree of sliding, we used the methods referenced by Tsukada et al.15) However, because no report on the radiographic measurement of femoral head rotation was found to the extent we could examine, detection of this parameter was performed using our original method.14)
The ability to stabilize femoral head rotation appeared to be greater with blade-type materials than with screw-type materials. Furthermore, we believe that a non-cylindrical blade is preferable to a cylindrical blade for the surgical treatment of the comminuted, unstable trochanteric fractures to prevent femoral head rotation and cut-out.








 XML Download
XML Download