

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Among fatigue fractures, a fracture caused by routine external forces due to the presence of a fragile bone such as osteoporosis are particularly referred to as insufficiency fracture. The major causative is postmenopausal osteoporosis; nevertheless, geriatric osteoporosis, adrenal cortical hormone treatments, and vitamin D deficiency may be also causatives. It occurs commonly in the thoracic vertebrae, the tibia, the fibula, and the calcaneus in most cases, however, insufficiency fracture of the femoral shaft has statusbeen reported recently. Therefore, we report the experience for the treatment of 16 femoral insufficiency fracture patients together with a review of the literature.
METHODS
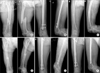
The study was conducted on a total 14 femoral insufficiency fracture patients treated at our hospital from July 1, 2002 to June 30, 2008. Two orthopaedic doctors diagnosed the patients as insufficiency fracture by the characteristic radiographic findings1) including femur lateral cortical hypertrophy, transverse fracture, and medial cortical beaking (Fig. 1). Among the 14 patients, 11 patients were admitted to the emergency room for injuries caused by weak lower extremities from injuries that developed from a misstep and fall due to standing or kneeling and the remaining 3 patients were admitted to the emergency room or through outpatient clinics for pain in the thigh or the inguinal area.
The mean age was 75.6 years (range, 65 to 89 years), and all patients (100%) were female. Also, all 14 female patients were postmenopausal women, and the mean menopausal time was 44 years (range, 35 to 52 years). The average weight of the 14 patients was 45.7 kg and the mean height was 147.3 cm. The mean follow-up period was 50.6 months (range, 14 to 86 months).
Cases with the risk factors of insufficiency fracture, having a history of using adrenal cortical hormones, renal failure, or using fluorine were excluded through a medical record review. In regards to the presence or absence of osteoporosis, the 14 patients performed dual-energy X-ray absorptiometry and the t-value of the hip as well as the vertebra was lower than -3. In addition, concerning the administration of osteoporosis agents issued recently, the type of drugs and the duration of medication were also examined.
Among 14 patients, 7 patients (50.0%) experienced predromal symptoms pain in the thigh as well as the inguinal area between 1 month and 4 months prior to injury, and among them, 3 patients visited other hospitals. Nonetheless, the diagnosis by pelvic plain radiography demonstrated no abnormality, and in 1 case, the patient had been given a misdiagnosis of intervertebral disc herniation by spinal magnetic resonance imaging.
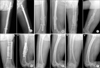
Among 14 patients, 11 patients were treated surgically (Fig. 2), and for 3 patients, only the follow-up observation was performed. Among the 11 patients who received surgical treatments, 2 patients, had surgery performed on the bilateral femurs, and bilateral fractures developed within approximately 5 years in one patient, and in approximately 4 months interval in the other patient. In the remaining 9 patients, surgery was performed on the one femur, and only the follow-up observation was performed on the contralateral side. Regarding the fixation of the femur, intramedullary nails were used in 9 patients (7 patients with unilateral and 2 patients with bilateral fracture, 11 cases), and plate fixation was performed in 3 patients (3 cases). The 3 patients who did not require surgery were the cases showing typical radiological characteristics on plain radiographs, which were lateral cortical hypertrophy as well as transverse fracture lines, and since pseudomotion caused by fracture were not detected, in all cases, weight bearing was reduced by the use of crutches, the outpatient follow-up observation was performed every 3 months, and plain radiography was performed (Table 1). In all patients who underwent surgery, bone union as well as fixation stability were assessed by taking plain radiography prior to surgery, immediately after surgery and at 6-week, 12-week, and 24-week intervals (Fig. 3). Bone union was assessed by 2 orthopedic surgeons, and if the opinion of the two specialists was not in agreement, it was determined by consulting with the 3rd orthopedic surgeon.
Through the application of medical records, a bone density examination, and radiographs, the level of osteoporosis, the fracture pattern, and bone union status were examined, and if required, telephone interviews were conducted.
For the mean weight and height of the Koreans, the Korean Agency for Technology and Statistics (KATS) website was referred, and for the average menopausal time, the statistics bureau (http://kostat.go.kr/portal/korea/index.action) website was referred. In regards to statistical analysis, one sample t-test and SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA) was used.
RESULTS
The mean body weight of the Koreans in the same age group was 58.1 ± 9.7 kg, and the mean height was 155.5 ± 8.8 cm. The mean body weight regarding our insufficiency fracture patients was 45.7 kg, and in comparison with the mean body weight of the same age group, it was statistically significantly lower (p < 0.001). The mean height was 147.3 cm and it was significantly shorter than the mean height of the Koreans in the same age group (p = 0.002) (Table 2). Insufficiency fracture patients showed statistically significant lower body weight and shorter stature than the general population. In regards to menopausal time, the mean menopausal time of the Koreans was 48.0 ± 4.2 years, being 44 ± 4.7 years in our study, and menopause occurred statistically significantly earlier (p = 0.017).
In terms of osteoporosis medication, the 11 patients (78.5%) were prescribed alendronate (8 pateints), pamidronate (2 patients), and risedronate (1 patient). The duration of medication was 1 to 8 years. Three patients remembered the medication but could not remember the drug or the medication period. However, among the entire 14 insufficiency fracture patients, 13 patients (92.8%) had a past history of osteoporosis and the experience of medication.
Among total 14 patients, 7 patients had predromal symptoms, and among the predromal symptoms, 6 patients experienced pain in the inguinal area (85.4%), 4 patients experienced pain in the thigh (57.1%), and 3 patients (42.9%) presented with pain in the inguinal area as well as pain in the thigh. Concerning the statistical significance between predromal symptoms and fracture, since the number of cases was small it was difficult to detect the association.
Among 11 cases using intramedullary nails, 3 cases (27%) showed delayed union, and thus additional surgeries such as bone graft, dynamization, and exchange of the intramedullary nail were required. Furthermore, among 2 plate fixation patients, in 1 case, metal failure occurred, nonunion was shown in 1 case, and thus bone graft and refixation using metal plates were performed, and 1 patient showed a somewhat stable union. Thus, while restricting weight bearing activities through the delay of walking with crutches, conventional treatments were performed, and ultimately, all fracture patients achieved union.
DISCUSSION
Insufficiency fracture in the femoral shaft or the proximal area caused by osteoporosis is not rare; however, numerous investigators have reported the association with the long term use of bisphosphonate in the past 3 years.1-7) In 2005, Odvina et al.5) reported that 9 patients used alendronate for longer than 3 years for the first time, and among them, 6 patients who had delayed union results, and in the histomorphometric study of bones, severely suppressed bone turnover was detected. Goh et al.2) have reported in a study conducted on 13 subtrochanter fracture patients caused by low energy injury that alendronate was administered for an average of 4.2 years (range, 2.5 to 5 years), and premonitory symptoms developed in 5 patients (56%) 2-6 months prior to fracture, pain in the inguinal area was developed in 1 patient, and pain in the lateral femur was developed in 4 patients. Neviaser et al.4) have reported in a study conducted on 70 subtrochanter and femur shaft fracture patients caused by low energy injury that in 25 patients who used alendronate for an average of 6.2 (range, 1 to 10) all cases showed the characteristic radiological results.
After the approval by the USA Food and Drug Administration in 1995, alendronate has been shown to reduce spinal or femoral fracture significantly in two randomized controlled studies,8,9) and presently, it is the first drug widely used for postmenopausal osteoporosis. Such alendronate induces apoptosis by reducing osteoclast activity resulting in the reduction of bone resorption,10) which increases bone mineral density ultimately, and suppresses bone turnover and thus reduces spinal or femur shaft fracture,8,11) however, Mashiba et al.3) have reported that it causes the accumulation of musculoskeletal microdamages in animal experiments. Similarly, Whyte et al.12) claimed that in humans, the continuous intravenous use of pamidronate causes the development of osteopetrosis or marble bone disease, and such microdamages eventually increase the risk factors of insufficiency fracture.
In our study, all 14 menopausal women experienced diverse osteoporosis medications. In terms of the types of osteoporosis drugs, in our study, alendronate was taken by 7 patients, pamidronate was taken by 2 patients, and risedronate was taken by 1 patient. Schneider6) has reported that in conclusion, it is not known whether all bisphosphonates reduce bone turnover or whether only alendronate becomes a problem.
Neviaser et al.4) claimed that body mass index was not associated statistically, Goh et al.2) claimed that higher incidence of insufficiency fracture occurred in younger women, nevertheless, studies on the factors that were suggested to be significant in our study such as underweight, short stature, and early menopause could not be found. Most osteoporosis drugs are excreted from the kidney, a small amount of drugs remaining in the body adhere to osteoid tissues, and react for several years.13) Regarding this process, it is considered that studies assessing whether an identical dose of an osteoporosis drug remains more in the body for underweight or short statured individuals or adheres better to ostoid tissues and its reactions are required.
In addition, delayed union or nonunion is frequent in insufficiency fracture. In our study, similarly, among 13 performed surgeries, in 5 cases (38.4%), incorrect union or nonunion was developed, and additional treatments such as additional bone graft, implant exchange, etc. were required. The causative of such delayed union or nonunion is not clear, and the causative may be inferred to be severe bone turnover induced by osteoporosis drugs.7) However, several investigators have reported that the union of fractured areas was obtained while using alendronate continuously, and thus it is considered that more studies on such delayed union and nonunion are required.
In our study, the long term administration of osteoporosis drugs and the cause as well as results of insufficiency fracture could not be established. Nonetheless, it is considered that in early menopause patients, underweight patients and short stature patients prescribed osteoporosis drugs for an extended period of time, it may be better to suspect femoral insufficiency fracture and to perform radiography or bone scan. Lastly, in order to fully understand the long term effects of osteoporosis drugs and whether or not it is a risk factor regarding insufficiency fracture, more cases as well as additional studies are required.



 XML Download
XML Download