

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer (BC) is one of the most common types of malignancies in women worldwide [1]. The incidence of BC has been increasing in several developing countries over the past few years including that among the Iranian women [23]. Epidemiologic studies implicate Western diet and the cultural transition toward Westernization of diet as plausible etiologic reasons for increased disease incidence [4]. However, there is controversy concerning the dietary components that should be reduced and the dietary modification that might contribute to the reduction of BC risk.
The findings of the European Prospective Investigation into Cancer and Nutrition cohort study suggested inverse associations between fruit and vegetable intake and BC risk [5]. Accordingly, other cohort studies similarly supported the protective role of vegetable intake and BC risk among women [6]. The risk of female breast carcinoma in association with the consumption of Allium vegetables was denoted in the Netherlands cohort study on diet and cancer, whereas a French epidemiologic study showed that higher onion intake as the most often consumed Allium vegetable was significantly correlated with a lower risk of BC [678]. However, there are rare and inconsistent results within most observational studies, indicating inverse associations between the intake of onion or other Allium vegetables and the risk of BC.
The anticancer effects of Allium vegetables are attributable to various organosulfur compounds [8]. Several studies showed that onion is the richest dietary source of quercetin [9]. Quercetin and other flavonoids are biologically active components with promising anticancer properties. Vitamin C is an active antioxidant rich in onion and other Allium vegetables [10]. Inulin and other oligofructoses are present in miscellaneous edible fruit and vegetables such as wheat, onion, garlic, and leeks [11]. There are many possible mechanisms through which dietary factors with prebiotic properties may play a protective role against the development of BC including the alteration of estrogen metabolism, as well as the antiproliferative and antioxidant effects [11]. In vitro and animal studies have shown that butyrate can regulate cell proliferation, and it is also capable of inducing differentiation and apoptosis in transformed tumor cells [11].
Although the protective role of Allium vegetables, particularly garlic and onion are often reported against gut-related malignancies [12]. Objectively, the possibility of such an association remains a preliminary question to be resolved. The common use of fresh and raw Allium vegetables in the Iranian diet provides an exceptional opportunity to understand the possible connection between fresh Allium consumption and BC risk. However, in humans, the evidence on whether Allium vegetables as prebiotic containing foods can prevent the development of BC is limited, which is overlooked and also detailed in experimental studies [1213]. Hence, the aim of the present hospital-based matched case-control study was to assess the association of dietary status of prebiotic containing foods with BC risk among Iranian women in northwest Iran.
METHODS
Study subjects
The present hospital-based case-control study was conducted from January 2012 to June 2013 at the private Shams Hospital in Tabriz, northwest Iran. In a consecutive case series, 310 eligible newly diagnosed BC participants were recruited from inpatient women who had been admitted to the surgery ward of the hospital [14]. They underwent partial or radical mastectomy. Of the 310 women, 285 were eventually histopathologically confirmed to have BC (grade II, III or clinical stage II, III, with invasive ductal carcinoma). The inclusion criteria were as follows: age of 25 to 65 years; no prior history of histologically confirmed malignancies; no previous history of cancer; no history of cystic abnormalities or benign breast disease; not a pregnant, postpartum, or breastfeeding mother (at the time of inclusion); following a specific dietary habit (vegetarian); not having disorders of polycystic ovary syndrome and chronic inflammatory disorders (colitis, gastritis, multiple sclerosis, lupus erythematosus, and severe rheumatologic disorders). The exclusion criteria were chronic use of methotrexate, sulfasalazine, anticonvulsants, and contraceptive drugs, and a body mass index (BMI) >45 kg/m2. History of benign tumors and not completing the interview (n=25) were the main reasons for excluding some of the BC cases (n=285). A written consent form was signed before the completion of the questionnaire by each participant who was assigned to either of the case or control groups. The study was approved by the Institutional Review Board of the Tabriz University of Medical Sciences (ethics number: 5/4/644). In addition, Tabriz is the capital city of Eastern-Azerbaijan, one of the crowded cities of northwest Iran. The Shams Hospital is a private hospital and one of the major referral centers for BC surgery from the neighboring provinces, including Ardabil, Western-Azerbaijan, Hamadan, and Kurdistan. Therefore, the residence statuses were matched between the cases and controls during study sampling. In parallel, 310 patients hospitalized at the same hospital for nonneoplastic diseases were considered eligible as the control group. Controls were matched to cases in a frequency of 1:1 based on age at diagnosis (5-year interval) and their residence statuses (rural/urban and/or province). Controls were chosen at the same seasonal time to avoid information bias regarding to seasonal changes. In this respect, the 5-year age interval was defined to improve the rate of sampling in the control group and matching performance for controls. The inclusion criteria for the participants of the control group were as follows: no prior history of malignancies and benign neoplasms, the will to participate in the study; not pregnant, postpartum, and breastfeeding mother; following a vegetarian diet and not affected by chronic inflammatory disorders (colitis, gastritis, multiple sclerosis, lupus erythematosus, and severe rheumatologic disorders).
The patients in both groups were interviewed face to face by two trained interviewers to complete a structured questionnaire on demographics (age, residence status, marital status, education level, and occupation); reproductive history, hormone use, family history of BC, and physical activity level. The body weight and height were self-reported at the time of the interview. Subsequently, the BMI was calculated as the body weight in kilograms divided by squared height in meters (kg/m2). The World Health Organization defined a BMI of 25 to 29.9 kg/m2 as overweight, and a BMI >29.9 kg/m2 as obese. Relevant medical information and histological findings were obtained from the hospital medical records.
Dietary assessment
Dietary data were collected using a detailed interviewer-administered food frequency questionnaire (FFQ) with 136 food items that were validated in our previous reports to contain certain nutrients [151617]. The intake frequency of each specific food item of Allium vegetables was asked to be defined as daily, weekly, monthly, and yearly. The frequency was multiplied by the intake measured in a regular household utensil in order to calculate the average daily intake of each Allium vegetable (g/day). Finally, standard reference values were used to convert the household portions to a unique unit of grams for each food [18]. The FFQ questionnaire was planned to record the consumptions of the previous year. Certain portion sizes were used for each food item to facilitate the conception of the amounts. The list of Allium vegetables present in the FFQ included the onion (cooked and raw), spring onion, watercress, cooked leek, local fresh green leaf of leak, garlic, and fresh leaves of garlic. When a food item from Allium group was consumed by more than 15% of study population, it was included in the present list of Allium vegetables. A set of color photographs showing fruits, vegetables, breads, and cereals was also used. In addition, the customary household utensils were considered to represent the average portion size for the other food items in order to minimize the interindividual variations. Seasonal variations of fruit and vegetables were also included in the statistical calculations. Moreover, a 3-day 24-hour dietary record was also used to test the accuracy of the data measured for dietary intake. In addition to the Allium vegetables, the dietary intake of other food items was included in the Nutritionist software IV for each participant version 3.5.2 (N-Squared Computing, San Bruno, USA) to calculate the estimated intake of total calories, macronutrients, and fiber.
Moreover, we analyzed two alternate categories based on consumption; consumers compared to the total population that included both the consumers and nonconsumers. Therefore, both classifications could predict the risk of exposure to food items that could increase disease susceptibility. Indeed, the main reason for performing the analyses in two distinct groups involving (1) the total population (cumulative data consisting of the consumers and nonconsumers) and (2) consumers of each food item separately, was to account for the probable skewness that could likely be introduced by the total population of women with BC who did not have any dietary intake of certain Allium vegetables. The estimates showed that 27% of the BC patients had not consumed one of the Allium food items, whereas the dietary habits of 20% of the controls did not contain one item out of all the Allium vegetables.
Statistical analysis
All statistical analyses were performed using the SPSS software 13.0 (SPSS Inc., Chicago, USA). The Kolmogorov-Smirnov test for the analysis of histograms was used to examine the normal distribution of continuous quantitative variables in subgroups, and box plots were generated to remove the outliers. When the data distribution was not normal, logarithm transformations of the data were conducted. If the data was still not normally distributed, the Mann-Whitney U-test was applied. Otherwise, the independent samples t-test was performed to compare the continuous variables between the case and control groups. The Pearson chi-square test was performed for categorical variables in association with BC development. The tertile stratification of dietary variables was undertaken based on the data available for the control population. Unconditional logistic regression analysis was performed to calculate the odds ratios (OR) and the corresponding 95% confidence intervals (CI) using the lowest quartile group as reference. Multivariate conditional logistic regression analysis was performed to include the related potential confounding factors in the adjusted models. All p-values were two-tailed and a p-value <0.05 was considered statistically significant.
RESULTS
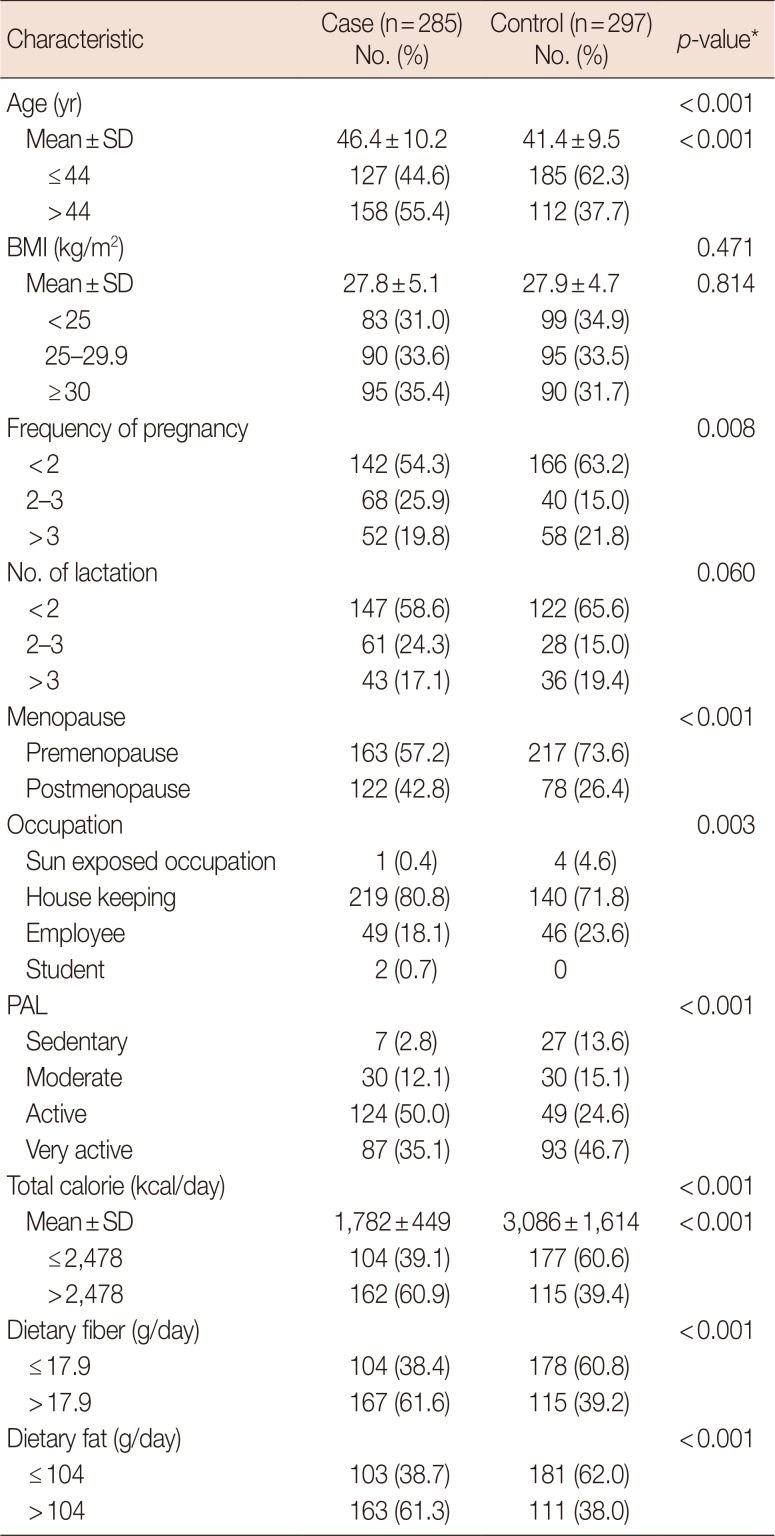
The general characteristics of 285 participants with BC in the case group and 297 age and region-matched hospital-based controls are demonstrated in Table 1. The mean age at diagnosis of BC patients was higher than the ages of the participants in the control group (46.4±10.2 years vs. 41.4±9.6 years, respectively; p<0.001). The frequency of >2 live childbirths was estimated to be higher in the BC group compared to that of the control group (p=0.008). Postmenopausal women were frequently observed in the BC group (p<0.001). Higher intakes of total calories, dietary fat, and fiber were frequently observed among the cases rather than the controls (p<0.001). Therefore, these independent physiologic and dietary variables were considered as covariates in the multivariate logistic regression analyses.
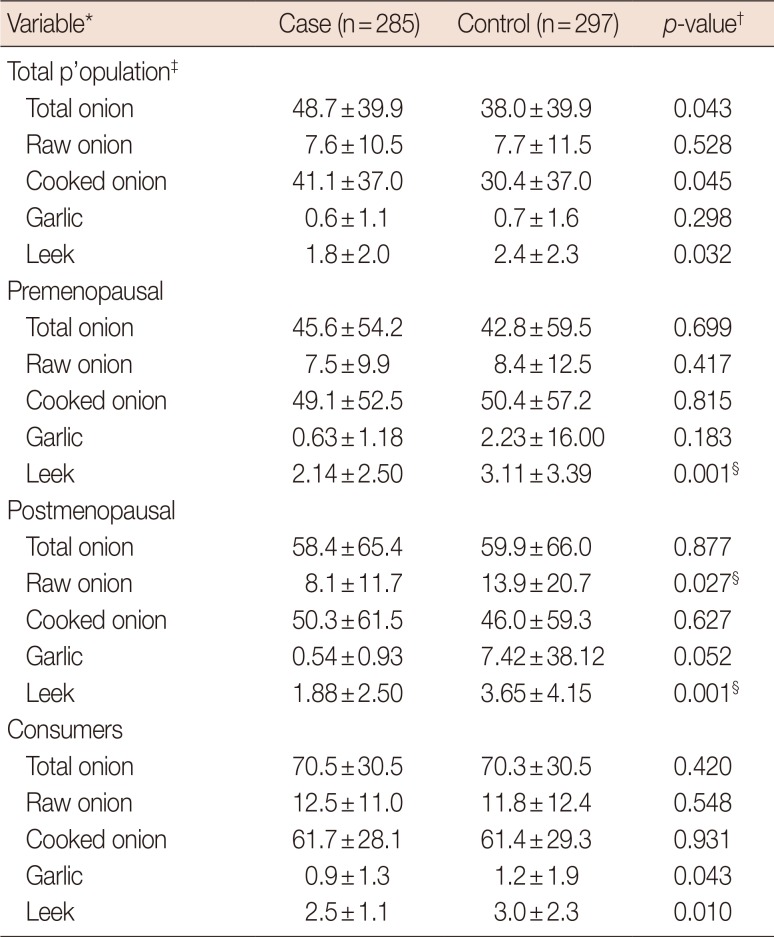
The average intake levels of Allium foods for the cases and controls are demonstrated in Table 2. Leek consumption was significantly higher in the controls (2.4±2.3 g/day) than that in the cases (1.8±2.0 g/day) for the total population (p=0.032), and similar results were obtained in the consumer population (p=0.010) and stratum of menopausal status (p=0.001). Participants in the case group consumed a higher amount of either variable of total (p=0.043) or cooked onion (p=0.045) compared to the controls in the total population. The mean daily consumption of garlic was also estimated to be higher in the control group that in the case group in the consumer population (p=0.043). The postmenopausal women with BC had a lower consumption of raw onion compared to the women in the control population (p=0.027).
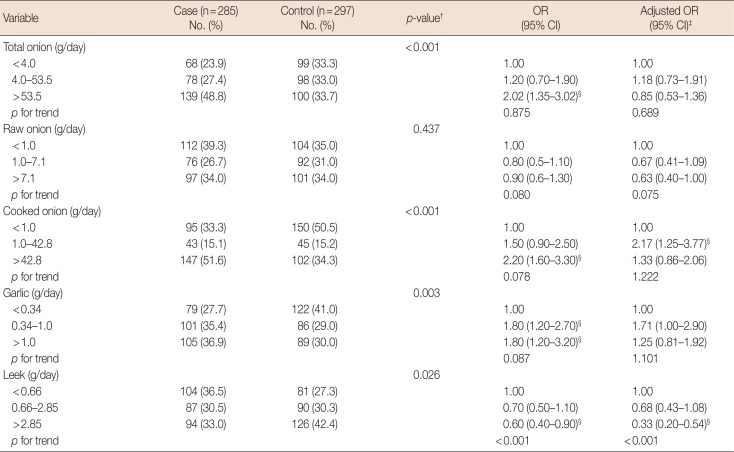
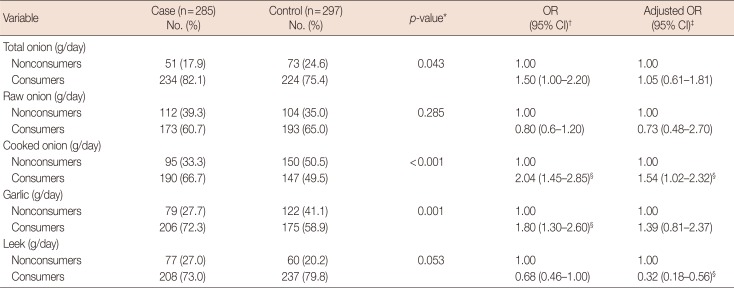
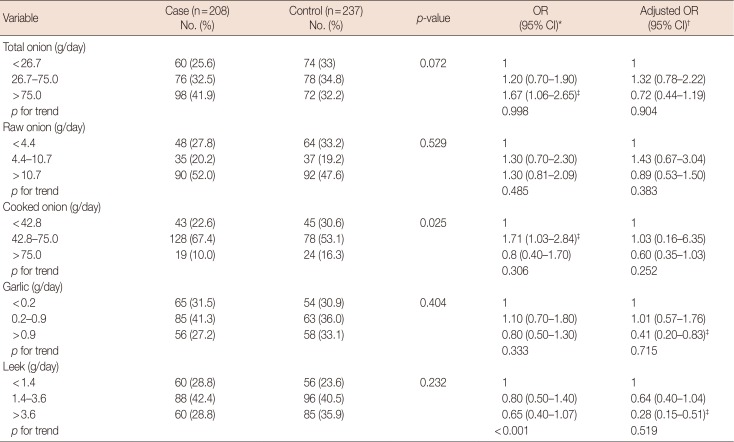
The association between the consumption of Allium vegetables (categorized variables based upon tertiles) and the risk of BC among both the cases and controls are demonstrated in Table 3 for the total population of consumers and nonconsumers and in Table 4 only for the population of consumers for each Allium vegetable. Although the findings from the present study showed that the consumption of raw onion was higher in the control group than that in the case group (Table 3), the protective effect of raw onion against BC development was estimated at an OR of 0.63 (95% CI, 0.40–1.00) after adjusting for potent covariates, and was statistically insignificant (Table 3). The consumption of cooked onion was higher in the case group (51.6%) than that in the control group (34.3%) for the total population (p<0.001). The high intake of cooked onion was associated with twice the risk of BC development (OR, 2.20; 95% CI, 1.60–3.30) (Table 3), compared to the reference lowest tertile. The type of cooked onion used in the consumer population included fried (52.2%), boiled (19.6%), and both boiled and fried onion (28.2%).
We observed that garlic was more frequently consumed in the case group (36.9%) than in the control group (30.0%) for the total population (p=0.003) (Table 4). The highest tertile of garlic consumption in the total population was correlated to an increased risk of BC (OR, 1.80; 95% CI, 1.30–2.60) (Table 5). Among only garlic consumers, the highest tertile of intake was notably associated with half the risk of BC development (95% CI, 0.20–0.83), when adjusted for effective confounders (Table 5). A higher intake of leek was associated with a significant reduction in the risk of BC for the highest tertile of consumption in the total population (OR, 0.6; 95% CI, 0.4–0.9) (Table 4). The consumers of leek after adjusting for covariates were at a lower risk of BC (OR, 0.32; 95% CI, 0.18–0.56) compared to the nonconsumers (Table 4). Among the consumers, the highest tertile of leek consumption was also associated with a lower estimated risk of BC development (OR, 0.28; 95% CI, 0.15–0.51) compared to the lowest intake category as reference (Table 5).
DISCUSSION
The present hospital-based case-control study was carried out among Iranian women with newly diagnosed BC in northwest Iran. To the best of our knowledge, the present investigation is the first to examine the potential effects of Allium vegetables such as onion, garlic, and leek on the risk of BC. Our main findings suggested that the consumption of garlic and leek was significantly associated with a lower risk of BC.
Moreover, our findings are consistent with those of experimental studies that reported the inhibitory role of several Allium-derived compounds on breast carcinogenesis [19]. The anticancer effects of Allium vegetables are attributable to the various organosulfur compounds [20]. However, findings from epidemiological data series were controversial concerning the associations of Allium vegetables and the risk of BC [21]. Onion stratification into either raw or cooked category appeared to notably attenuate the effect of cooking. Our findings showed that the higher tertile of cooked onion consumption was significantly correlated to an increased risk of BC. These findings were also persistent after adjusting for possible effective confounders. Consistent with our findings, a case-control study conducted in Uruguay by Ronco et al. [22] demonstrated that both raw and cooked vegetables were inversely associated with the risk of BC irrespective of the low consumption of raw vegetables (one-third to one-half less than cooked vegetables). Accordingly, Franceschi et al. [23] conducted a large case-control study on women with BC in six different Italian areas and showed that a high intake of raw vegetables could be associated with a reduced risk of BC, whereas the consumption of cooked vegetables was not significantly associated with the risk of BC. In a case-control study on women with BC in the German population [24], similar findings were obtained, supporting an inverse association between the intake of raw and total vegetables and the risk of BC; however, increased intake of cooked vegetables showed no significance. Collectively, these findings suggest that the consumption of raw vegetables is more often inversely associated with the risk of BC compared to the consumption of cooked vegetables. Similarly, Bao et al. [7] showed in a large case-control study that the intake of Allium vegetables was correlated with the risk of BC in the Chinese population. Irrespective of the fact that the mechanisms behind the different physiological effects of raw and cooked vegetable consumption and the risk of BC are unclear, the inconsistency of evidence might partly be explained by the type of cooking described as boiled or fried. Fried onion was the prominent type of cooked onion recorded often in the habitual diet of the Iranian population [25], and even among the BC population, in contrast to the boiled onion prominently used in the Western population [26]. Consuming high dietary fat along with fried onion could notably interfere with the main effect of analysis between cooked onion and increased risk of BC. In addition, cooking decreases water solubility and attenuates the activity of heat-sensitive functional components, e.g., flavonoids [27]. Irrespective of our findings that failed to show the statistically significant beneficial effects of daily raw onion consumption on the risk of BC, one can assume that the cumulative amount of total onion consumption was also underscored by the relative frequency of using cooked onion concerning the risk assessment for breast carcinogenesis.
The dietary intake of raw local leek was associated with a reduced risk of BC in the present study. The Netherlands Cohort Study conducted in the Dutch population by Dorant et al. [21] showed that the high dietary intake frequencies of onion and leek were not associated with the risk of BC. Similarly, a hospital-based case-control study in the Greek population with no intake categorization of onion and leek showed no significant correlation to the risk of BC. It is conceivable that information biases, seasonal variations and possible misclassifications might be taken into consideration when analyzing inconclusive evidence concerning the relationship between high leek consumption and the risk of BC [21].
The anticarcinogenic effects of Allium vegetables are supported by several case-control studies conducted in patients having other malignancies [28]. The dose-response preventive effects of garlic and onion intake on the development of disease in different anatomic sites of the gut, particularly gastric and colorectal cancers, might be attributable to the direct exposure to anticarcinogenic compounds in Allium vegetables [13]. Breast carcinogenesis might be indirectly influenced by the chemopreventive effects of Allium components owing to the interfering pharmacokinetic effects of their metabolic variables and absorption boundaries [29].
Our analyses among garlic consumers showed that the highest tertile of garlic consumption could be associated with half the amount of risk of BC in the case group compared to the control group. Accordingly, findings from a case-control study conducted among French women showed an inverse association between garlic consumption and the risk of BC [8]. Generally, the Mediterranean dietary habits are followed among the French population, containing cooked garlic in combination with tomato or olive as seasoning [8]. The intake of fresh and raw garlic is a customary dietary habit and is highly combined with Iranian meals and side dishes. Thus, the present study provided an exclusive opportunity to assess the possible preventive effect of fresh garlic on the risk of BC risk. In addition to oligofructose components, garlic is a rich food item containing organosulfur-derived active reagents largely considered to prevent carcinogenesis through the improvement of the cellular immune system function, induction of the xenobiotic metabolizing enzymes that detoxify mutagens (by stimulating glutathione synthesis), reduction of nitrosamine production and its metabolic activation, suppression of the covalent binding of 7,12-dimethylbenz[a]anthracene to DNA, and the induction of apoptosis and cell cycle arrest [7]. In another study, Henderson and Feigelson [30] suggested that the effect of using garlic on the risk of BC could partly depend on the possible changes in hormonal factors. Moreover, the relative frequency of garlic consumption combined with the consumption of other Allium vegetables or whole vegetables in daily meal that could be effective in protecting against the risk of cancer should be studied in nested-case control studies.
There were some limitations in the present study. The limited sample size in some strata could not support categorization based on menopausal or pathological status. The recall bias is a consequence of the imprecise nature of retrospective dietary assessment; however, in an attempt to minimize the potential effects within random errors, we ascertained estimated portion sizes as well. Furthermore, our FFQ was validated for particular related nutrients especially folate that is an abundant nutrient in many fruits and vegetables [151617]. In addition to adjusting for several established BC risk factors, we also adjusted for the total energy intake to take the subjects' tendency of over- or under-reporting into consideration. However, there might still be potential for differential recall based on the awareness of disease status. Moreover, residual confounding might mask the true association between the consumption of Allium vegetables and the risk of BC owing to the inability to control total fruit and vegetable intake.
The results collectively obtained from the consumer and whole populations almost showed the same trend of ORs in tertiles. Thereby, both classifications consistently predicted the risk of disease susceptibility based on the consumption of Allium vegetables. Nonetheless, as observational studies cannot separate the effect of food constituents from the effects of other unidentified components in vegetables and fruits, it is plausible that our findings might be interpreted as an effect of customary dietary habits among the present sample population of Iranian women with BC.
In conclusion, our hospital-based case-control study showed protective associations between the consumption of specific Allium vegetables and the risk of BC. However, additional epidemiological studies should be conducted in a large cohort to confirm the protective effects of garlic and onion against BC according to menopausal and/or pathological status. Our findings could help pave the way for other cohort or nested case-control investigations concerning the investigation of dietary Allium vegetables as low-cost remedies that could prevent the incidence of BC among the high-risk populations.
 XML Download
XML Download