

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Even though controversy remains, concerning the necessity of internal mammary lymph nodes (IMN) irradiation for breast cancer patients [1], several studies have presented results showing that IMN irradiation decreased the risk of locoregional recurrence and improved survival [2-4]. Still, many physicians are concerned about the IMN irradiation, since it may increase the exposure of radiation to critical organs, such as lung and heart [5]; they are also skeptical of the efficacy of IMN irradiation. Clinical practice for IMN irradiation has depended on the physician's discretion, and varied widely by hospital and country [6]. The patterns of the care study for post-mastectomy radiotherapy in Korea showed that 48% of breast cancer patients received IMN irradiation [7]. This controversy could be resolved when further evidence will be obtained by the results from large prospective clinical trials, such as the European Organization for Research and Treatment of Cancer (EORTC) 22922/10925 trial and the National Cancer Institute of Canada Clinical Trials Group (NCIC-CTG) MA.20 trial [8,9]. In Korea, a multi-center trial, the Korean Radiation Oncology Group 08-06, was launched in 2008. Interim analysis of NCIC-CTG MA.20 trial, with a median follow-up of 62 months, showed that the addition of regional lymph node irradiation improved disease-free survival with the tendency of improved overall survival, but increased grade 2 or greater pneumonitis (1.3% vs. 0.2%) [10]. The toxicity until 3 years after the treatment of the EORTC trial reported significantly increased lung toxicity in the IMN treatment group (4.3% vs. 1.3%), but the clinical impact of the increased lung toxicity was minimal [11].
Various techniques are available for breast cancer radiotherapy with IMN irradiation [12-17]. The partially wide tangent field technique (PWT) is one of the techniques used to include the IMN, in addition to the whole breast for radiotherapy after breast conservation surgery (BCS) [18]. We previously investigated the optimal radiotherapy technique for irradiating IMN with the whole breast after breast conservation surgery, by comparing the plans using planning techniques, including the standard tangent field, wide tangent field, PWT, and photon-electron mixed field. We found that PWT was the best technique in terms of coverage of IMN and reduction of the lung and heart dose [19].
Radiation pneumonitis (RP) is a common toxicity caused by radiation exposure to the lung, and the incidence of RP is known to be correlated with the volume of the irradiated lung and the radiation dose. The mean lung dose and V20 (percentage of lung volume that received a dose of 20 Gy or more) are generally related to RP [20]. Kwa et al. [21] reported that the mean lung dose could be useful in predicting the risk of RP, through an analysis of 540 patients, including 59 breast cancer patients. However, the exact relationship between dosimetric parameters and RP has not yet been fully established in breast cancer treatment [21,22]. Central lung distance was used as an indicator for the prediction of RP before the advent of 3-dimensional conformal radiotherapy (3D CRT) planning. However, there is no guideline for planning breast cancer radiotherapy to prevent RP in the 3D CRT planning era.
At our institution, IMN and supraclaviclular lymph nodes (SCL) have been included in the radiotherapy field after BCS for patients with a medial tumor or positive axillary lymph nodes (clinical or pathologic N stage ≥1) since 2004. Most patients were treated with PWT. A small group of patients was treated with photon-electron mixed technique. Based on early experience, with the first 20 patients, we decided to treat IMN with PWT in patients whose normal tissue complication probability (NTCP) of ipsilateral lung was less than 45% [23].
The purpose of this study was to evaluate the risk of RP in terms of dosimetric parameters in breast cancer patients who received radiotherapy with PWT after BCS.
METHODS
Patient selection
Between September 2004 and August 2009, a total of 108 breast cancer patients underwent 3D CRT, using PWT after BCS at the Yonsei Cancer Center, Severance Hospital and Gangnam Severance Hospital. After a review of the medical records, 100 patients who had undergone a chest X-ray within 6 months of radiotherapy completion were included in this study. This study was approved by the institutional review board of our institution (IRB approval No. 4-2012-0532).
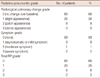
The patients were all female, and the median age was 48 (range, 27-70). The Eastern Cooperative Oncology Group (ECOG) performance score was 0 for all the patients. None of the patients had a history of smoking or pulmonary disease. Of the 100 patients, 54% were treated for right breast cancer and 46% were treated for left breast cancer. Sixty-seven patients had a tumor in the inner quadrant, 31 patients had a tumor in the outer quadrant, and the tumor locations of the two patients were unknown. Eighty percent of tumors were histologically confirmed as ductal carcinoma. Two patients had SCL involvement with tissue confirmation, but none of the patients had IMN involvement. Patient distributions by the clinical stage were 45 in stage I, 41 in II, and 14 in III. Sixty-one patients were pathologic stage N0, 23 were stage N1, 6 were N2, and 10 were N3. None of the patient had metastasis.
Seventy-three patients received chemotherapy, including 20 patients receiving concurrent chemo-radiotherapy (CCRT) after the operation. Detailed treatment characteristics are shown in Table 1.
Radiotherapy planning
For simulation, a computed tomography (CT) scan was performed in all patients in the supine position with the ipsilateral arm in abduction on a customized immobilization device. The acquired CT images with 5 mm spacing were transferred to the treatment planning system (Pinnacle3; Philips Medical System, Andover, USA) for radiotherapy planning. The breast tissue, SCL, IMN were delineated as target volumes, and the ipsilateral lung, heart, vocal cord, and esophagus were also contoured as critical organs on the CT images for each patient. The entire breast and IMN were irradiated with a total dose of 50.4 Gy in 28 fractions, using a 6 MV linear accelerator and the PWT. The tangent fields of PWT were planned to cover IMN located in the first three intercostal spaces, as well as the entire breast. SCL was irradiated by a separate beam, which was designed not to overlap with the breast field; 50.4 Gy in 28 fractions was prescribed to 3 cm depth for SCL. The field arrangement is shown in Figure 1.
Radiation pneumonitis assessment
Follow-up visits for physical examination and chest X-ray were scheduled 1 month after the completion of radiotherapy, and then 3 to 6 months, thereafter. To examine the radiological pulmonary changes, chest X-ray images obtained within 6 months after radiotherapy were compared to those obtained before the start of radiotherapy. Radiological changes, only in the SCL field, were not counted as RP. Symptoms related to RP, such as cough or exertional dyspnea, were identified and recorded at all the follow-up visits.
RP was scored, according to the Radiation Therapy Oncology Group/EORTC toxicity criteria, i.e., grade 0=no change over baseline; 1=asymptomatic or mild symptoms (dry cough), slight radiographic appearances; 2=moderate symptomatic fibrosis or pneumonitis (severe cough), low grade fever, patch radiographic appearances; 3=severe symptomatic fibrosis or pneumonitis, dense radiographic appearance; 4=severe respiratory insufficiency/continuous O2/assisted ventilation; 5=death. Grades for each of the radiologic changes and symptoms were recorded, and the total RP grade was designated as the higher grade of the two.
Dosimetric parameters and statistical analysis
The dosimetric parameters, used in the analysis, were the mean ipsilateral lung dose (MLD), V5, V10, V20, V30, V40, V45, V50, and NTCP. For NTCP calculation for the ipsilateral lung, the coefficients of n (volume effect), m (slope), and TD50 (tolerance dose), based on Lyman-Kutcher-Burmann model were 0.87, 0.18, and 24.5 Gy, respectively [24].
The correlations between RP and the parameters were analyzed by t-test, Pearson chi-square test, and Fisher's exact test. Receiver operating characteristic (ROC) curve was used to determine the cut-off values to evaluate the predictive ability of dosimetric parameters. Statistical analysis was carried out, using PASW Statistics version 17.0 (SPSS Inc., Chicago, USA). A p<0.05 was considered statistically significant.
RESULTS
Incidence of radiation pneumonitis
Of the 100 patients, 66 did not develop any radiologic changes or symptoms related to RP. The total RP grade of 1 occurred in 26 patients, grade 2 in six patients, and grade 3 in two patients. No one developed total RP grade 4 or 5. Radiologic changes were noted in 26 patients with grade 1, and in eight patients with grade 2. On the other hand, eight patients experienced a mild dry cough (grade 1 symptom), which subsided spontaneously. Only three patients suffered from clinically significant symptoms (grade ≥2 symptoms, symptomatic RP), and among those who did, steroids were prescribed in two patients, due to severe cough (Table 2). The characteristics of the patients who had a total RP grade of ≥2 are summarized in Table 3.
Relationship between radiation pneumonitis and treatment regimen
Seventy-three patients received chemotherapy, sequentially (n=53) or concurrently (n=20). Among these 73 patients, RP developed in 26 patients, including eight who received CCRT. Among the eight patients having grade 1 symptoms, chemotherapy was performed, sequentially, in three patients, and concurrently in two. One patient suffering from grade 2 symptoms received CCRT. There were two patients with grade 3 symptoms, and among them, one patient received sequential chemotherapy. However, administration of chemotherapy did not correlate with incidence of RP, regardless of grade.
Sixty-seven patients received hormone therapy, and six patients had a total RP grade of ≥2, including two patients with symptomatic RP. Only six patients received targeted therapy, but none of them had total RP grade of ≥2. There was also no significant correlation between the treatment regimen and incidence of RP.
Relationship between radiation pneumonitis and dosimetric parameters
The ranges of MLD and NTCP, in all patients, were 6.6 to 24.3 Gy and 0% to 76%, respectively. Ninety-five patients had NTCP of less than 45%. Even though total RP grade of 1 is not clinically significant, we included patients with total RP grade 1 in the analysis, due to the small incidence of total RP grade of ≥2.
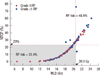
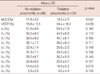
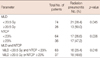
Univariate analysis showed that MLD and NTCP were significantly different between total RP grade 0 and grade ≥1 (p=0.042 and p=0.029, respectively) (Table 4). MLD of 20.5 Gy and NTCP of 23% were determined, as the cut-off points for the incidence of RP, using an ROC curve. RP incidence was 50% in patients with MLD ≥20.5 Gy, but 28.4% in those with MLD <20.5 Gy (p=0.045). RP incidence was also higher in patients with NTCP ≥23% than in those with NTCP <23% (47.2% vs. 26.6%, p=0.036). RP occurred more frequently in the group with MLD ≥20.5 Gy or NTCP ≥23% (18/37, 48.6%) than in the group with MLD <20.5 Gy and NTCP <23% (16/63, 25.4%), which is illustrated in Figure 2. This difference was statistically significant (p=0.018). The correlation between the incidence of RP and dosimetric parameters, however, is mostly suitable to predict radiological changes, not for symptomatic RP, since only 11 patients had any symptoms (Table 5).
There was no dosimetric parameter that was statistically correlated with total RP grade ≥2. In patients who developed total RP grade ≥2, MLD and NTCP varied considerably, ranging from 15 to 24.3 Gy and 3% to 76%, respectively. RP involving clinically significant symptoms occurred in three patients, who had MLD of 16.6, 17.6, 20.5 Gy. Also, NTCP for these three symptomatic RP patients ranged from 6% to 28%. The average value of V20, known as the greatest predictor for RP for lung cancer, was not different between symptomatic RP (37.7±4.9%) and asymptomatic RP (grade ≤1 symptoms) patients (36.8±7.3%).
DISCUSSION
We analyzed the correlation between dosimetric parameters and the incidence of RP in breast cancer patients, who received radiotherapy, using PWT after BCS. The incidence of RP, including asymptomatic minimal pulmonary radiologic change or mild dry cough, was higher in patients with MLD ≥20.5 Gy or NTCP ≥23%. Symptomatic RP occurred in 3 (3%) of the 100 patients. These patients were relieved by supportive care, meaning observation or corticosteroids. Since the incidence of symptomatic RP was too low, there were no significant predictive factors in dosimetric parameters for RP.
RP generally appears within 6 months from the completion of radiotherapy. Its incidence after whole breast irradiation, without a nodal irradiation, is known to be 1% to 2% [25-27]. Lingos et al. [25] reported in 1991 that 1% of symptomatic RP incidence (17 out of 1,624) in breast cancer patients received radiotherapy with tangent fields alone, or with tangents and SCL or SC-axillary region irradiation. SC-axillary region irradiation and chemotherapy increased the occurrence of RP (3.3%). Kim et al. [28] reported that the incidence of symptomatic RP, after whole breast and SCL nodal region irradiation, was 2.3%, which was higher than 1.7% of the incidence after whole breast irradiation alone. However, they did not apply the IMN irradiation. In our study, symptomatic RP occurred in three patients (3%). Despite the use of PWT to include IMN irradiation, RP incidence, in our study, was not higher than that of the other studies. Thus, we suggest that the PWT technique is a feasible option that does not increase the risk of RP when treating the whole breast, including the IMN.
Even though the risk of RP is known to correlate with radiation dose and irradiated lung volume, the relationship has not been fully studied in breast cancer patients. Krengli et al. [29] suggested that minimizing V25 to 100 cm3 could reduce the grade of pulmonary changes detected by high-resolution computed tomography in 41 patients. Lind et al. [30] reported that ipsilateral V20 could predict the risk of pulmonary toxicity by analyzing 128 patients using the ROC curves. We previously reported the dosimetric parameters to predict RP for breast cancer patients by analyzing 20 BCS patients treated with PWT (n=17) and the photon/electron mixed technique (n=3) [23]. This previous study concluded that less than 45% ipsilateral lung NTCP would prevent RP. However, this previous study determined this predictive parameter using only radiologic changes, since only one patient who received CCRT suffered from symptomatic RP. Also, due to the small amount of data, we could not come to a definite conclusion. This study was a data analysis of 100 patients, including 17 patients from a previous study, who received radiotherapy using PWT. We obtained statistically meaningful dosimetric parameters to predominantly predict radiologic changes. Since only three patients suffered from grade ≥2 symptoms, among the total 100 patients, it was difficult to obtain any statistically meaningful results for symptomatic RP. Therefore, a larger pool of patient data is needed to establish clinically meaningful dosimetric parameters that predict RP.
Our study had some limitations. There was a possibility that the toxicity evaluation was incomplete, since this was a retrospective study. However, as toxicities were evaluated at the 1, 3, and 6-month follow-up visits after radiotherapy, most RP was noticed, especially when symptoms were involved. Second, more thorough examination could be achieved by using a chest CT. However, because a chest CT is not routinely examined in our institution, due to the risk of secondary malignancy, we reviewed a radiological change with a chest X-ray taken within 6 months, post-radiotherapy. Third, NTCP calculated in this study could be overestimated, as NTCP for the only ipsilateral lung was calculated using the coefficients n, m, and TD50, based on the Lyman-Kutcher-Burmann NTCP model, which was obtained for pneumonitis in bilateral lung [24]. With the use of a more precise model for predicting ipsilateral lung complications, more meaningful predictive NTCP value could be obtained.
The dosimetric parameters obtained, in this study (20.5 Gy of MLD and 23% of NTCP), may be useful as a reference for reducing the risk of RP. However, these values seem too low to practice clinically, and the original protocol, NTCP <45%, can be applied for clinical practice when PWT is used. As seen in this study, symptomatic RP could occur in patients with low NTCP values (6%), possibly based on individual differences in lung sensitivity to radiation. Therefore, within 6 months, the time in which the RP can develop, after the completion of radiotherapy, all patients should be carefully followed-up so that supportive care can be provided immediately in the event of RP.
In summary, our data showed the incidence of RP, including asymptomatic radiologic change, to be correlated with dosimetric parameters of NTCP and MLD, but the clinical impact was minimal. However, we suggest that PWT is a safe technique for treating IMN in BCS patients with very low risk of symptomatic RP, when NTCP is less than 45%. Further studies using larger sample sizes are needed to address useful dosimetric parameters for predicting symptomatic RP.



 XML Download
XML Download