

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A family history of breast cancer is a well-established, strong risk factor for breast cancer [1]. Previous studies suggest that a family history of breast cancer also increases the risk of breast cancer recurrence and the risk of the second primary breast cancer [2345]. A majority of these studies have investigated the associations between mutations in BRCA1 and BRCA2 genes and the risk of breast cancer recurrence and contralateral breast cancer [5]. However, mutations in BRCA1 and BRCA2 are found only in about 6% to 23% of patients with breast cancer with a family history, suggesting that other genetic factors may contribute to a family history of breast cancer [67]. Among these factors, other DNA repair genes have received increased attention [8]. Impaired DNA repair capacity in individuals with certain genetic variations in DNA repair genes results in slower rates of DNA damage repair caused by endogenous and exogenous influences, thus increasing cancer risk [8].
Among the risk factors that induce DNA damage, ionizing radiation has been long recognized as a breast cancer risk factor [9]. Some studies also suggest that the association between ionizing radiation and breast cancer risk is stronger in women with a family history of breast cancer as compared to women without a family history [1011]. On the other hand, because of the sensitivity of malignant breast tissue to the effects of ionizing radiation, radiotherapy has been widely used for the treatment of patients with breast cancer. Some concerns have been raised regarding the potential damaging effects of radiation therapy on the surrounding normal tissue and the tissue in unaffected breast. Recognizing this concern, previous studies have been conducted to investigate the association of radiation therapy with the risk of local (ipsilateral) recurrence and the risk of contralateral breast cancer. While radiotherapy has been reported to decrease the risk of local recurrence [51213], the risk of contralateral breast cancer has been found to increase after radiotherapy, especially in younger women [512141516]. To date, only one study examined the impact of a family history of breast cancer on the relationship between radiotherapy and the risk of contralateral breast cancer [14]. This study found a significant additive interaction between radiotherapy and a positive family history of breast cancer in relation to the risk of contralateral breast cancer [14]. Two studies also examined the association between a family history of breast cancer and the risk of local recurrence in women treated with radiotherapy. These studies had relatively small samples, and did not find significant associations [1718]. The purpose of the current study was to examine the association between a family history of breast cancer and the risk of breast cancer recurrence in women who received or did not receive radiotherapy in an established breast cancer registry.
METHODS
Study population and data collection
The Breast Cancer Registry of Greater Cincinnati (BCRGC) was established by the University of Cincinnati, Department of Environmental Health in 2003. The registry aims to collect information on incident and prevalent breast cancer cases in the Greater Cincinnati area and to explore the risk factors for breast cancer in this population. Women and men living in the Greater Cincinnati area and diagnosed with breast cancer are recruited through local oncology practices, media, and community outreach events. The women in the registry represent a volunteer convenience sample. Demographic information, clinical characteristics of the tumor (except tumor size and stage), treatment history, reproductive history, and detailed family history of cancer are collected via the baseline self-administered questionnaire. The data in the registry are available for analyses conducted by approved investigators at the following link: http://eh.uc.edu/breastcancerregistry/researchers/index.html.
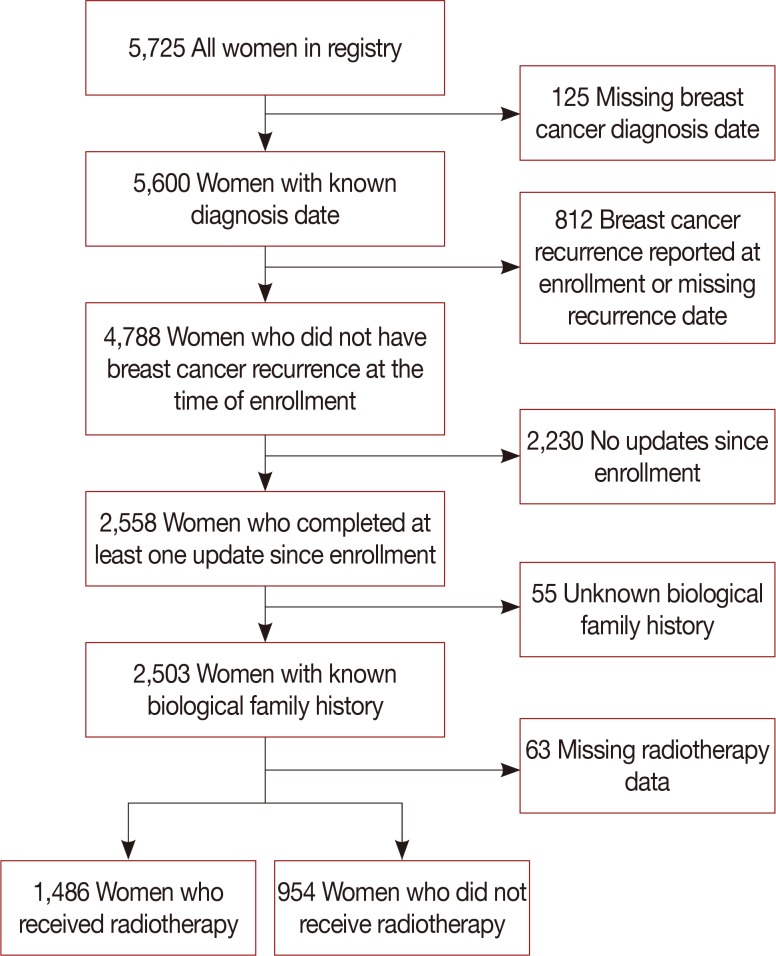
The data on recurrence of the tumor and updated information on breast cancer risk factors used in this analysis were collected in 2006, 2011, and 2013. Out of 5,725 women in the BCRGC, we excluded women with missing diagnosis date (n=125) and women with a prior history of breast cancer recurrence or missing recurrence date at enrollment (n=812). To be eligible for the study, women were required to have at least one update completed during the follow-up and to have knowledge of their biological family history (n=2,503). We further excluded women with missing radiotherapy history information (n=63). The final study sample included 2,440 women (42.6% of all participants in the BCRGC), of which 1,486 had a history of receiving radiotherapy and 954 women did not receive radiotherapy (Figure 1). Of these women, 41.3% were incident breast cancer cases and 58.7% were prevalent cases. Characteristics of women in the study sample were similar to characteristics of all women in the registry. The average follow-up time between the initial and the first available update questionnaire, and between the initial and the last available update questionnaire, were 2 years (range, <1–8 years) and 4 years (range, <1–10 years), respectively. This study was approved by the University of Florida and University of Cincinnati Institutional Review Boards (protocol numbers 201400996 and 20123745, respectively). All women provided written informed consent.
Radiotherapy and family history of breast cancer
Information about radiotherapy for the initial breast cancer diagnosis was collected at baseline. Detailed information on a family history of breast cancer in first- (mother, sister, and daughter) and second-degree relatives (paternal and maternal grandmothers and aunts) was collected at baseline and updated at each follow-up cycle. As inherited genetic susceptibility may not have fully manifested at the time of entry into the study, we supplemented data on family history from baseline with the updates to fully capture this information. For these analyses, a family history of breast cancer was defined in several ways: (1) having any first-degree relative with breast cancer diagnosis (any or none); (2) total number of first-degree relatives with breast cancer; (3) total number of relatives with breast cancer; and (4) a total family history score that was calculated as the sum of the number of first-degree relatives with breast cancer and half the number of second-degree relatives with breast cancer.
Covariates
Information on potential confounders was collected at baseline and updated throughout the follow-up period. These confounders included age (years) and body mass index (BMI, kg/m2) at the time of diagnosis, menopausal status and postmenopausal hormone use (premenopausal, postmenopausal who never used hormones, postmenopausal with hormone use history, and postmenopausal with unknown hormone use status), a history of benign breast biopsies (yes/no), parity and the age at first birth (nulliparous, any children with age at first birth <25 years, and any children with age at first birth of ≥25 years), a history of alcohol consumption (any/none), and smoking (yes/no). We further examined the following factors related to breast cancer diagnosis and treatment: receptor status (positive or negative for estrogen receptor [ER], progesterone receptor, and human epidermal growth factor receptor 2), nodal involvement (positive/negative), and a history of surgery (yes/no), chemotherapy (yes/no), and adjuvant hormone therapy (yes/no).
Statistical analysis
Distributions of baseline characteristics in women with and without a history of radiotherapy were compared using the t-test (for continuous variables) and chi-square test (for categorical variables). To compare characteristics of women in the study sample and all women in the registry, we first created a new indicator variable explaining whether the population represents that of the entire registry or of the study sample in respective data sets. Next, two data sets (entire registry and study sample) were combined into one and the distribution of variables by the indicator variable described above was compared using the t-test or chi-square test.
Cox proportional hazards models with time since diagnosis in months as the underlying time variable were used to calculate hazard ratios (HRs) and the corresponding 95% confidence intervals (CIs). The primary endpoint, breast cancer recurrence, was defined as an episode of recurrence self-reported on any of the update questionnaires. For individuals with breast cancer recurrence, follow-up began at the time of breast cancer diagnosis and ended on the date of breast cancer recurrence. If the exact date of recurrence was not specified, the mid-point between the previous contact and the date of the update when the recurrence was reported was used as the estimated date of recurrence (n=10). For women without breast cancer recurrence, follow-up began at the time of diagnosis and ended at the time of the last contact or at the end of the study (December 31, 2014), whichever occurred first. As age and BMI have shown significant associations with breast cancer-free survival in previous studies [219], both of these variables were forced into the survival models. The best fitting model was selected using step-wise model selection approach and only covariates that met statistical significance at 0.05 level were kept in the final models. The survival models were run separately for each of the family history variables in women who received and did not receive radiotherapy.
The proportional hazards assumption was tested for the survival models within each of the radiotherapy strata. The results suggested no assumption violations (among women with radiotherapy, proportionality test p-values ranged 0.730–0.915; among women with no radiotherapy, proportionality test p-values ranged 0.206–0.569). The differences in the associations between each of the family history variables and the risk of breast cancer recurrence in women who received and did not receive radiotherapy were tested by including an interaction term in the survival model for the entire study sample.
In a secondary analysis, to examine the potential influence of immortality bias, we defined the start of the follow-up time for women with prevalent breast cancer as the date of recruitment rather than breast cancer diagnosis. In additional analysis, we also excluded 10 women with unknown exact dates of recurrence during the follow-up. Finally, to determine if the type of surgery might influence our findings, we explored the influence of the type of surgery in the analysis (modeled as mastectomy, breast-conserving surgery, or no surgery). The findings with this modeling approach were very similar to those obtained with binary history of surgery variable. As the binary modeling approach provided better data balance, the history of surgery was modeled as yes versus no in all the analyses. All the tests were two-sided and significance of the effects was assessed at the 0.05 level. All analyses were performed using SAS statistical software version 9.4 (SAS Institute Inc., Cary, USA).
RESULTS
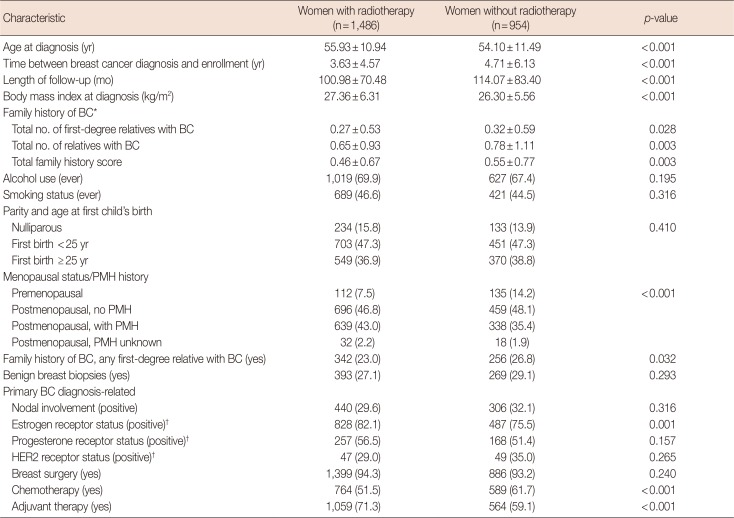
This study included 2,440 women with breast cancer (1,486 who received radiotherapy and 954 who did not receive radiotherapy). The average follow-up time was 8.42 years for women with radiotherapy (median, 7.27; interquartile range [IQR], 3.91–11.50) and 9.51 years for women without radiotherapy (median, 7.90; IQR, 4.23–13.29). During the follow-up, there were 109 reported recurrences (69 in women with radiotherapy and 40 in women without radiotherapy). The distribution of selected characteristics among study participants by the status of radiotherapy is presented in the Table 1.
Compared to the participants without radiotherapy, women who received radiotherapy were older (55.93 years vs. 54.10 years, p<0.001), had greater BMI (27.36 kg/m2 vs. 26.30 kg/m2, p<0.001) at the time of breast cancer diagnosis, had a smaller total number of first-degree relatives with breast cancer (0.27 vs. 0.32, p=0.028), were less likely to have any first-degree relative with breast cancer (23.0% vs. 26.8%, p=0.032), and were less likely to have a history of chemotherapy (51.5% vs. 61.7%, p<0.001). There was also a significant difference in women's menopausal status and postmenopausal hormone use between the two groups; women who received radiotherapy were more likely to be postmenopausal and to have a history of postmenopausal hormone use (p<0.001). The distributions of other characteristics were similar in women with and without radiotherapy.
In univariate analysis of the associations of age, BMI, tumor characteristics and clinical variables with the risk of recurrence in women with and without radiotherapy, BMI and surgery were the only variables that were significantly associated with the risk of recurrence in both strata (BMI ≥25 to <30 kg/m2 vs. <25 kg/m2 [HR, 2.84; 95% CI, 1.47–5.50] and BMI ≥30 kg/m2 vs. <20 kg/m2 [HR, 4.03; 95% CI, 2.10–7.74] for women with radiotherapy; BMI ≥25 to <30 kg/m2 vs. <25 kg/m2 [HR, 2.21; 95% CI, 1.01–4.85] and BMI ≥30 kg/m2 vs. <20 kg/m2 [HR, 2.62; 95% CI, 1.05–6.52] for women without radiotherapy; surgery yes vs. no [HR, 0.12; 95% CI, 0.07–0.19] for women with radiotherapy; surgery yes vs. no [HR, 0.11; 95% CI, 0.06–0.22] for women without radiotherapy). Among women with radiotherapy, ER negative status was also associated with an increased risk of recurrence (ER– vs. ER+: HR, 2.20; 95% CI, 1.22–3.97), but this association was no longer significant after adjustment for other covariates in the full model.
The results of the survival analysis in women with and without a history of radiotherapy are summarized in Table 2. Among women with a history of radiotherapy, breast cancer recurrence was not associated with any of the variables for the family history of breast cancer after adjustment for age and BMI at diagnosis and a history of surgery (any first-degree relative with breast cancer: HR, 0.98; 95% CI, 0.58–1.68; total first-degree relatives with breast cancer: HR, 0.89; 95% CI, 0.57–1.39; total number of relatives with breast cancer: HR, 0.96; 95% CI, 0.75–1.23; total family history score: HR, 0.92; 95% CI, 0.65–1.32).
Among women without a history of radiotherapy, the total number of relatives with breast cancer was positively associated with breast cancer recurrence, with approximately a 21% increase in the risk of recurrence per any additional family member with breast cancer (HR, 1.21; 95% CI, 1.00–1.47). None of the other family history variables were associated with the risk of breast cancer recurrence in women without radiotherapy. The risk estimates for any of the family history variables did not differ significantly across the radiotherapy strata (p-interaction >0.05 for all).
In a secondary analysis with the start of the follow-up defined as the enrollment date for women with prevalent breast cancer, the results remained unchanged (data not shown). Similarly, the results did not change after exclusion of 10 women with unknown exact date of recurrence (data not shown).
DISCUSSION
We examined the interactions between radiotherapy and a family history of breast cancer in relation to the risk of breast cancer recurrence in an established prospective breast cancer registry. Our findings suggest no difference in the associations of the family history of breast cancer with the risk of breast cancer recurrence by the status of radiotherapy.
Consistent with previous reports, we found no association between a family history of breast cancer and the risk of breast cancer recurrence among women who received radiotherapy [1718]. Chabner et al. [17] found no association between a family history of breast cancer in first-degree relatives and the risk of local recurrence among 201 women diagnosed with stage I or II invasive breast cancer and receiving radiotherapy. Similarly, a case-control study in women with early-stage breast cancer receiving breast-conserving surgery and radiotherapy did not find any association between a family history of breast cancer and breast cancer recurrence among 52 women with a local recurrence and 52 matched controls [18].
We found a significant association between the total number of relatives with breast cancer and the risk of breast cancer recurrence among women who did not receive radiotherapy. The results from previous studies on a family history of breast cancer and the risk of recurrence are inconsistent [2021222324]. A retrospective study by Turkoz et al. [24] reported an increased recurrence risk among family history-positive breast cancer cases with young age or triple negative breast cancer (HR=1.62 and 1.82, respectively). Similarly, Jobsen et al. [23] found a positive association between a family history of breast cancer and the risk of local recurrence among young breast cancer patients (age ≤40 years old). However, three cohort studies found no association between the family history of breast cancer and/or ovarian cancer and the risk of breast cancer recurrence [202122].
Our study utilized an established prospective cohort with more than 12 years of follow-up. Women included in the analysis were representative of all women in the registry with respect to important characteristics. In addition, characteristics of women in the registry and in the analysis were similar to those from previous studies [25]. Unlike previous studies, we defined a family history of breast cancer using various approaches, which allowed us to separately examine the effects of the family history in first-degree relatives, family history in both first and second-degree relatives, as well as a total score that accounted for the nature of these familial relationships. It is possible, however, that some of the effects were not detected due to the relatively small number of recurrences in this cohort. Information on breast cancer risk factors, tumor characteristics, treatment history, and breast cancer recurrence status was self-reported and misclassification of the recurrence status cannot be excluded completely. However, previous studies suggest high accuracy of self-reported cancer history, history of breast cancer recurrence, and treatment [2627]. A previous study reported high agreement between self-reported data (recall time, 1.6–9.0 years; mean, 3.2 years) and data in medical records; the agreement between the two data sources was 99% for a history of radiotherapy and 97% for breast cancer recurrence status [27]. The prospective data collection in our study also minimizes the possibility of misclassification. We could not, however, separately examine the associations for contralateral versus ipsilateral recurrence as this information was not available.
Our study population appears to be representative of breast cancer cases reported by the Surveillance, Epidemiology, and End Results Program with respect to the distribution of receptor statuses [28]. However, the registry did not collect information on breast cancer stage and tumor size. As treatment regimens are based on these tumor features and as we examined the effect of treatment history in our analysis (surgery, adjuvant hormone therapy, and chemotherapy), it is very unlikely that the absence of information on tumor stage influenced our findings. Even though information on the age at breast cancer diagnosis for first- and second-degree relatives was collected at enrollment, a substantial proportion of participants had missing data on these variables. Thus, we could not consider a younger age at diagnosis in modeling the family history in our analysis. Finally, as the follow-up time starts on the date of diagnosis rather than on the date of enrollment in the registry, the immortal bias is possible. However, as the average time between diagnosis and enrollment date was 4.0 years (median, 2.0; IQR, 0.6–5.2), which falls within the expected time window for observing recurrences, it is unlikely that the results were influenced by this bias. This is further supported by similar findings of the secondary analysis, in which the start of the follow-up for prevalent cases was set to the date of enrollment.
Some previous studies suggest that breast cancer patients with a positive family history of breast cancer tend to undergo cancer screening more frequently and from a younger age [29]. Higher dose and early age at exposure to ionizing radiation have been linked to breast cancer risk in previous studies [30]. Mammography represents a source of medical ionizing radiation in women and it is possible that the cumulative exposure to this radiation in women with a family history of breast cancer might contribute to a higher risk of breast cancer recurrence. Information on the number of prior mammograms, however, was not collected by the registry and could not be controlled for in this analysis. Similarly, the information on radiotherapy dose was also unavailable. Future studies would benefit from inclusion of this important information in the analysis, which would allow to account for a woman's total cumulative exposure to ionizing radiation.
In conclusion, our findings do not support the hypothesis that radiotherapy in breast cancer cases with a family history of breast cancer might increase the risk of breast cancer recurrence. Future studies are warranted to further examine these associations in larger population-based studies with complete information on ionizing radiation from prior mammography screening. If these findings are replicated by future studies, the results could be translated into an important health message to breast cancer survivors with a family history of breast cancer explaining that they are not at an increased risk of breast cancer recurrence due to the radiation exposure from their treatment as compared to women with no family history of breast cancer.

 XML Download
XML Download