

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dental ceramics are one of the most popular restorative materials in prosthodontics because of their natural and esthetic appearance, low heat conduction, good hygienic properties, and wear resistance. Despite many advantages, dental ceramics have some disadvantages in physical properties, such as low flexural strength and antagonistic natural tooth wear. Another popular esthetic restorative material in dentistry is composites. Comparing the brittle and rigid structures of the ceramics with composites, composites are less brittle. However, low color stability and higher wear of composites limit their use. Many existing disadvantages of the most popular dental restorative materials led to an effort to develop new biomaterials mimicking the physical properties of natural tooth in dentistry. Polymer infiltrated ceramic network (PICN) materials, also called hybrid ceramics, are current materials to overcome the present disadvantages of the ceramics and composites.1 Expected physical properties of the PICN materials are lower brittleness, higher flexural strength with rigidity, high strength, and easy milling in CAD/CAM system.2 The other physical features of PICN materials are similar to those of natural tooth structure and causing less tooth wear than dental ceramics.3
The long term aim of the PICN materials is mimicking natural tooth physical properties completely. A new PICN material "VITA Enamic" blocks (VITA Zahnfabrik, Germany), following this objective, has been available in the dental market since 2013.4 Since VITA Enamic is a novel PICN material in the dental market, there are limited knowledge and a limited number of dental literatures about their physical properties.1234 Shade matching and surface roughness are two important features of the restorative materials that determine the clinical success of the dental restorations including VITA Enamic. Thus, the aim of the present study was to investigate the change in surface roughness and color difference caused by different surface treatments of a new PICN material VITA Enamic.
MATERIALS AND METHODS
For all specimens, color 2M2 High Translucent (HT) and Translucent (T) VITA Enamic (Vita Zahnfabrik, Germany) blocks were chosen. A total of 120 rectangular specimens (2 × 12 × 10 mm) were prepared. After the production (Cerec, Sirona Dental System GmbH, Bensheim, Germany) all specimens were ultrasonically cleaned in distilled water and additionally cleaned with isopropanol to remove the residue, then dried with compressed air. VITA Enamic has its own three different surface finishing and polishing systems. The finishing and polishing systems suggested by VITA Enamic CAD/CAM blocks were Technical Kit, Clinical Kit, and VITA Enamic Glaze. The prepared specimens were divided into 8 groups as below to perform three different finishing and polishing procedures on each of the groups:
Control HT: The HT group - none of the surface finishing procedures were performed on it
Control T: The T group - none of the surface finishing procedures were performed on it
Group 1: The HT group - the surface finishing procedure was performed using Technical Kit
Group 2: The HT group - the surface finishing procedure was performed using Clinical Kit
Group 3: The HT group - the surface finishing procedure was performed with VITA Enamic Glaze
Group 4: The T group - the surface finishing procedure was performed using Technical Kit
Group 5: The T group - the surface finishing procedure was performed using Clinical Kit
Group 6: The T group - the surface finishing procedure was performed with VITA Enamic Glaze
For each group, the specimens were finished and polished subsequently using by a series of different Enamic burs. The Control HT and Control T groups did not go through any of the finishing and polishing procedures. The specimens of Groups 1 and 4 underwent the Technical Kit finishing procedure. Polishing instruments were applied with constant stroking motions in a single direction under dry conditions. First, Group 1 specimens were polished using by the silicon carbide pink rubber disc of the Technical Kit with 10.000 rpm hand piece (NSK, Tokyo, Japan). After the use of the pink rubber disc, the grey disc of the Technical Kit with smaller particle size was used with 5000 rpm (NSK, Tokyo, Japan), as suggested by the manufacturer.
For Group 2 and 5, VITA Enamic Clinical Kit was used. The finishing and polishing of the specimens were done with clinical handpiece instead of high-speed laboratory motor. Clinical Kit was applied to the Groups 2 and 5 using KaVo 500 Contra Angula and KaVo 500 Micro Motor (KaVo Porte Genuina, KaVo Brasil Industria e Comercio LTDA, Santa Catarina, Brazil) with a speed of 10,000 min-1 for the first step (with the pre-polishing pink rubber disc) and 5000 min-1 for the second step (with the high gloss polishing grey disc), as suggested by the manufacturer.
Glazing of the specimens was performed with VITA Enamic Glaze according to procedure recommended by the manufacturer. For Group 3 and 6, the first step of the surface finishing was made with the pink rubber of the laboratory kit. Then, VITA Enamic Glaze was used with LED polymerization unit (VALO LED, Ultradent Products Inc., South Jordan, UT, USA), as suggested by the manufacturer. Each of the specimens was polymerized for 20 seconds. The wavelength of the LED polymerization device used for the polymerization of Enamic Glaze solution was 395-480 nm. The definitive thicknesses of the all specimens were measured with a digital micrometer (Mitutoyo Corporation, Tokyo, Japan).
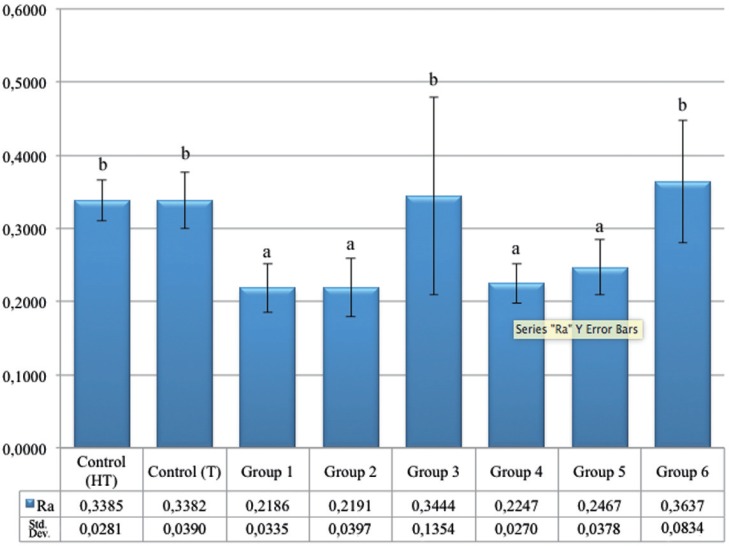
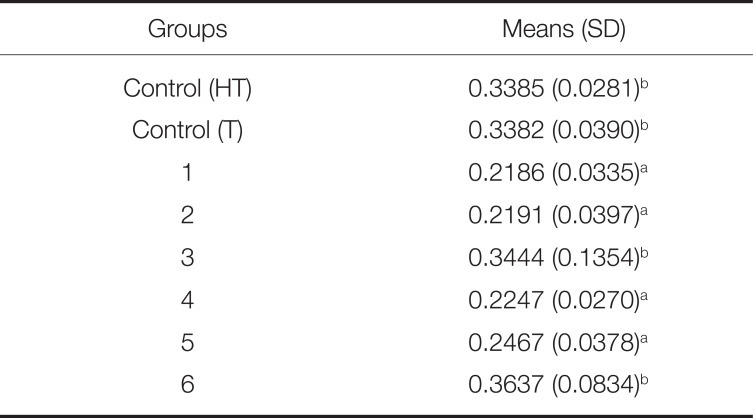
The surface roughness of the specimens was measured using a tactile profilometer (Surftest SJ 201, Mitutoyo, Tokyo, Japan) with a 0.25-mm cutoff value. The resolution of the profilometer was 0.01 mm with the transverse length of 4.0 mm and the diamond recording pin stylus diameter of 5 µm. The constant measuring speed of 0.5 mm/sec was used to determine an average roughness profile. Six measurements were made with equal distances (1.5 mm) on each specimen; the reading direction was always perpendicular to the finished surface of the specimens. The measured roughness parameter was Ra (arithmetical average value of all absolute distances of the roughness profile).
Color parameters were obtained with a portable spectrophotometer (VITA Easyshade Advance, VITA Zahnfabrik, Cuxhaven, Germany). The calibration of the device was made before each measurement. All the measurements were made in tooth single mod. Color measurements were performed before and after the finishing and polishing procedures to determine the color change of the specimens.
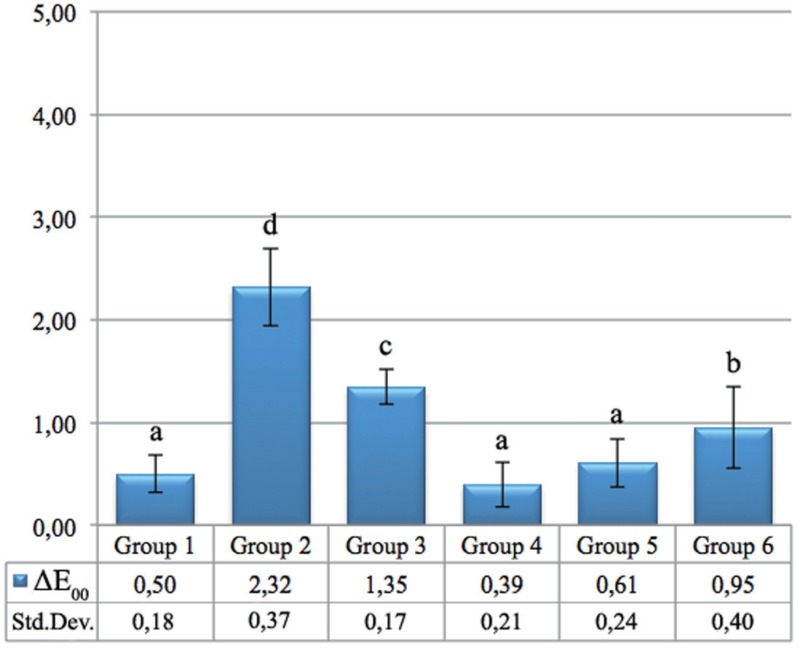
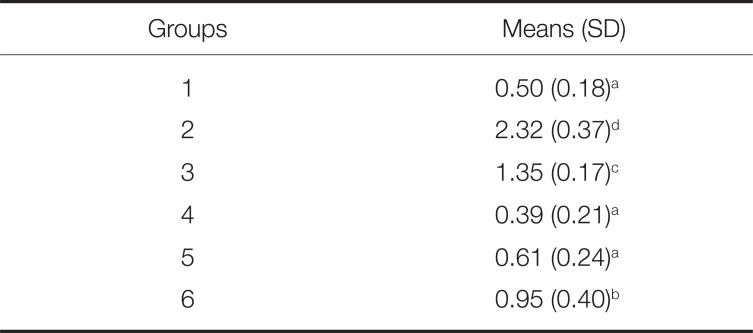
Color differences from before and after the finishing and polishing procedures were evaluated by CIEDE2000 system. For the present study, the clinically acceptable threshold of color difference value was considered to be 2.25 for ΔE00.5 Color differences ΔE00 greater than 2.25 were considered as perceivable differences for observer.
RESULTS
The mean and standard deviation of surface roughness values are presented in Table 1 and Fig. 1. The highest surface roughness values were observed in Group 3 and 6, which were glaze-applied study groups. Group 3 and 6 showed surface roughness values similar to Control HT and T. There were statistically significant differences between the Group 1, 2, 4, 6 and the Control HT, Control T, Group 3, 4 (P < .05).
Table 2 and Fig. 2 show the shade differences (ΔE00) between the groups after the three different finishing and polishing procedures. The highest difference was observed in Group 2, which was the 'high translucent' and Clinical Kit-applied group. There was no statistically significant difference between Group 1, 4 and 5. All groups except Group 2 demonstrated imperceivable shade difference by observer (ΔE00< 2.25) after the finishing and polishing procedures. Group 2 showed 2.32 ΔE00 value, which is a perceivable color change by an observer but not acceptable in dental clinical practice.
DISCUSSION
One of the most popular current topics in prosthodontics is CAD/CAM technique and related materials. The main reason for the popularity of CAD/CAM and related materials are time consuming feature of technique. Ease of operation and homogenous-almost flawless materials that technique uses to make restorations are another advantages of the CAD/CAM. Permanent non-metal CAD/CAM dental restorations are mainly divided into two groups: composites and ceramics. Although composites are compliant materials, composites are prone to wear because of their soft nature. On the other hand, ceramics are rigid and brittle materials causing antagonistic natural tooth to wear. Because these popular materials have the mentioned disadvantages, there is still an effort to accomplish an ideal restorative material similar to natural tooth's physical and optical properties. As a part of this effort, new polymer infiltrated ceramic network (PICN) materials were developed. PICN materials consist of two continuous interpenetrating networks. One network is of ceramic material and the other a polymer.6 The goals of PICN materials are reduced brittleness, greater rigidity and hardness coupled with improved flexibility, and larger fracture toughness and better machinability compared to ceramics.7
Also improvements of PICN maintain the wear "kindness" toward enamel of opposite tooth similar to composites. The long-term aim of PICN materials is the imitation of natural tooth structure.6 It was shown that VITA Enamic had better internal and marginal adaptation than feldspathic ceramics.8 This may be due to the good machinability of VITA Enamic with CAD/CAM.
To fulfill the demand of dentists to work independently of technicians, the clinicians should be well aware of the CAD/CAM and the physical properties of the related materials. However, the knowledge and dental literature about the effect of different finishing procedures on VITA Enamic color was limited because the material was unfamiliar in the dental market. Coldea et al.2 showed that the PICN materials tested in their study were more damage-tolerant than commonly used dental ceramics.
The finishing and polishing kits of the present study are quite similar to each other since both Technical and Clinical Kits include silicon carbide rubber burs. However, the difference between the Technical Kit and Clinical Kit is found in the dimensions of the burs and the finishing and polishing devices. Clinical Kit was applied with a clinical handpiece, but Technical Kit was applied with a laboratory micromotor. The types and trademarks of the finishing and polishing devices used in the present study are shown in the Materials and Methods section.
Accuracy of tooth color choice is important especially for non-metal restorations because the main aim of the restorations is esthetics and color match. The reason for popularity of current dental ceramics and other tooth-like dental materials may be the predictability of the final shade of restorations made from these materials. In prosthetic dentistry, shade determination is routinely performed visually with the aid of shade guides.9 Clinically applicable digital devices for shade determination, such as colorimeters and spectrophotometers for example, have also been introduced to enable objective shade selection. In the present study, a spectrophotometer and a tactile profilometer, both popular for measuring color and surface roughness, were used. A dental spectrophotometer (VITA Easyshade® Advance, Vita Zahnfabrik, Germany) was used in Tooth Single mode to record the CIELAB coordinates (L*, a* and b*) of the ceramic samples. The main objective to effort the shade selection of esthetic restorations is color matching between esthetic restorations and natural dentition. However, failure of color match between final restorations and natural dentition is not a rare condition because of the factors affecting the final color of the restorations.10
ΔE is the numerical distance between the L*a*b* coordinates of two colors, and it represents the color difference value. The clinically acceptable limit of color difference value is considered to be 2.25 ΔE00 units. The hypothesis of the present study was that different finishing and polishing procedures might affect the optical and physical properties of the CAD/CAM materials. Thus, in the present study, the effects of different finishing procedures on color and surface roughness of the Vita Enamic were investigated. Because of the unfamiliarity of the hybrid ceramics, there is not enough knowledge about the effects of finishing and polishing procedures on the shade matching of the hybrid ceramics. According to the results of the present study, the greatest shade difference before and after the finishing and polishing was observed in the Clinical Kit-applied Group 2. Group 2 was the 'high translucent' group to which the surface finishing procedure was performed using the Clinical Kit. The results of the Clinical Kit-applied 'translucent' group (Group 5) showed clinically accepted shade change (ΔE00< 2.25) after the finishing and polishing procedure. Although both Group 2 and 5 were finished and polished using Clinical Kit, the difference might be due to the effect of high translucency of the material on the final shade. Except for Group 2, which showed the highest ΔE00 unit (2.32), all the other groups showed clinically acceptable shade differences. Within the limitations of the present study, it may be suggested that all the finishing and polishing procedures except using Clinical Kit for high translucent material may lead to clinically acceptable shade matching.
Monasky and Taylor11 emphasized that porcelain with rough surface caused more tooth wear than smooth surface. Jung et al.12 reported less wear of the antagonistic teeth against zirconia than against dental porcelain, with the reason attributed to the smoother surface of zirconia. Surface roughness of dental materials are investigated widely in dental literature since surface roughness also affects surface free energy.13141516 It means that rough surfaces of dental materials cause a high surface free energy resulting in more microbial plaque formation.17 Thus, surface roughness of dental restorative materials is important because these materials are in contact with gingiva, the most critical area of oral environment. Rough surfaces of dental materials near the gingiva make a suitable location for microbial accumulation. Adversely, smooth surfaces of dental materials may cause easy surface cleaning and less microbial accumulation. It means that the surface roughness of the materials has importance related to the long term clinical performance of the dental restorations. Thus, in the present study, the surface roughness of the VITA Enamic was investigated. In the present study, glaze material was applied to the specimens directly, and then light curing device was used afterwards. According to the results of the study, glazeapplied groups (Group 3 and 6) showed the highest surface roughness value. Within the limitations of the present study, it may be suggested that finishing the VITA Enamic restorations using Clinical and Technical Kit instead of glaze results in smoother material surfaces. Regarding the shade matching after finishing and polishing, Clinical Kitapplied 'high translucent' group showed clinically perceivable shade change. Thus, according to the results of the present study, it may be suggested that finishing the VITA Enamic restorations using Technical Kit instead of Glaze and Clinical Kit gives better clinical performance in the aspects of both surface roughness and shade matching. Clinical Kit may be useful for minor corrections such as polishing the pre-adjusted occlusal surfaces intraorally in dental clinics. However, there is a need for further studies investigating the same parameters in vivo.
 XML Download
XML Download