

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
For intraoral scanners (IOS) to prevail over the conventional method, they must be easy-to-use and more efficient devices, and, especially, they must provide more accurate dental impressions for any restoration case. Accuracy is a requirement in any dental specialty, although it is certain that in some particular cases, the maximum allowable deviations are more restrictive. Prosthodontics is one of these specialties in which accuracy requirements are most demanding. This means that restorations fabricated from digital impressions must fit without causing any long-term clinical complications, i.e. with passive fit.1 So far, the limits of the passive fit have been analyzed in several studies, using different methodologies and measuring the admissible deviation in various directions.2345678
In dental implants, regardless of these limits, implant-supported reconstructions typically require a greater level of fit than teeth-supported reconstructions.9 Dental implants have reduced mobility and the lack of a periodontal ligament makes it impossible to adapt the implant to the poorly-adjusted framework; as a result, the implant and the framework are stressed.10 Accordingly, the goal of this work is to fabricate accurate restorations from digital impressions acquired with intraoral scanner (IOS). For that purpose, IOS must provide a reliable replica that will fit passively in the patient's mouth.
The development of IOS sought to overcome the challenges related to conventionally taken dental impressions, such as volumetric changes of impression materials, expansion of plaster models, or others related to the impression-taking process, such as improper tray selection, separation of impression material from the tray, or problems arising from the storage of impressions for the potential remaking of models.111213 By overcoming these challenges, within a few years IOS have increased their presence significantly.14 IOS and CAD/CAM already provide a more efficient way to perform restorations and have a higher acceptance rate among patients.151617181920
However, the practice of conventional impressions still persists. The validity of restorations made using IOS has been questioned from the beginning and many studies have been carried out to analyze their accuracy. Some have tried to directly assess the accuracy of IOS by performing studies in vitro.212223242526 Others have compared, also in vitro, digital impressions with conventional ones in larger areas such as a bridge or the complete arch111527282930 or have compared conventionally or digitally-performed restorations.3132333435363738
All these studies have been performed using different methodologies, in varying lengths of arch, considering different conditions of the patient, such as edentulous or toothed, and even with different versions of the same IOS.2439 These provided dentists and developers with varying results.
However, there is clearly a lack of accuracy studies performed in vivo. In this sense, when determining the accuracy of digital impressions, it is necessary to measure their trueness. The measurement of trueness has been the main obstacle in performing accuracy studies in vivo, even to the point of considering it impossible because of the difficulty to obtain references for trueness measurements.33343540
The aim of this research was to design a new methodology that enables the study of the accuracy of digital impressions in vivo - a methodology based on the use of a pattern that allows the assessment of both trueness and precision in distance and angle measurements. Simultaneously, this methodology allows analysis of the accuracy in different lengths of dental arch. For this purpose, the methodology has been tested to assess the accuracy, in terms of trueness and precision, of three different IOS.
MATERIALS AND METHODS
The basis of the proposed methodology was to measure from digital impressions achieved with different IOS in a specifically designed pattern. This pattern was previously measured in a coordinate measuring machine (CMM) to obtain control distances and angles.
The pattern design had to meet three requirements: 1) the size and shape had to be suitable for replicating the study in different arch models; 2) the pattern had to be valid for measuring distance and angle errors along the complete arch; 3) the material had to be dimensionally stable and biocompatible to enable in vivo replication of the study if the methodology used was validated.
To fulfill the size and shape requirement, digital impressions of five upper jaws were used. The goal was to design a pattern that would fit in as many jaws as possible without interfering with dentition. For that purpose, five plaster models were randomly chosen and digitized with a blue light technology based industrial reference scanner (Camera resolution of 2 × 5,000,000 pixels and distance between points of 0.017 mm – 0.481 mm) (ATOS Compact Scan 5 M/300, GOM). From this digitization, five digital impressions in standard tessellation language (STL) were achieved. The jaws were completely dentate and without any diagnosed pathology. The five digital impressions of the upper jaws were aligned and overlapped using reverse engineering software (Geomagic Design X with 2016.2.2 software version) to define the space in which the designed pattern should fit. Then, the structure of the pattern was designed and five cylinders were digitally placed along the pattern in order to obtain useful geometries for both distance measurements and, using their axes, angle measurements. A reference plane was also machined as a base geometry for further measurements The position of each cylinder corresponded approximately (depending on the characteristics of each jaw) to those of the maxillary right third molar, maxillary right canine, central maxillary incisors, maxillary left canine, and maxillary left third molar. Placing these reference cylinders along the pattern allowed the measurement of the distance and angle error along the complete arch. Then, the reference pattern was designed and fabricated in stainless steel (Fig. 1). The surface of the pattern was shot-blasted to avoid glare and reflections that can interfere with the scanning process.
Four distances between the five cylinders and the angles of each cylinder were defined (D12, D13, D14, D15 and A1, A2, A3, A4, A5) for measurement and error analysis. Accuracy was evaluated in terms of trueness and precision. Trueness was assessed as the deviation of measured parameters (distance and angle) in IOS digital impressions from control ones and precision, as the deviation of each measurement of reference parameters in these digital impressions. In both cases, mean and standard deviation were calculated using statistical analysis software (IBM SPSS Statistics 24, IBM Corp., Armonk, NY, USA).
The pattern was placed and fixed on a plaster replica of the upper jaw using light-polymerizing resin (CONLIGHT, Kuss Dental, Madrid, Spain). Afterwards, the model with the pattern was scanned 10 times with each of the three selected IOS (n = 30): iTero Element1 (Hereafter iTero) (Align Technology Inc., San Jose, CA, USA) with 1.5.0.361 software version; Trios3, (3 Shape A/S) with 2015-1 software version; and True Definition (3M ESPE, St. Paul, MN, USA) with 5.1.1 software version. In all scans, the complete arch was digitized together with the five cylinders of the pattern (Fig. 2). All the scans were performed according to the IOS manufacturer's scanning protocols for complete arch. When the scans were performed with the iTero or Trios3, the scanning began in the maxillary right first molar, and when performed with the True Definition, the scanning began in the maxillary right canine. All scans (n = 30) were performed by the same technician, in the same clinic and under the same temperature and humidity conditions. The first scans were performed using the iTero and Trios3. Afterwards, when scanning with True Definition, the model with the pattern was powdered (Lava COS Powder, 3 M ESPE), as in clinical practice and following the manufacturer's recommendations.
The defined four distances and five angles of the pattern were measured first using a CMM (CRYSTA-Apex S, Mitutoyo) and assessed as control. These four distances and five angles were also measured from each digital impression obtained with the IOS (n = 30) and compared with the controls. The measurements were performed using 3D inspection and mesh processing software for dimensional analysis (GOM Inspect with 2018 software version), following a specifically-designed measuring protocol.
To measure the 4 reference distances, 5 points were created in each cylinder of all STL files as the intersection between a cylinder axis and a plane. The reference distances were defined by linking these points (D12, D13, D14, and D15) (Fig. 3). The cylinders were created on each part of the mesh resembling a cylinder according to the Gaussian best-fit method. The software (GOM Inspect) squares the deviations of the selected polygons with the possible fitting element and adds the quadratic deviations. To create the intersection plane, firstly, the surface of the mesh corresponding to the horizontal plane of the pattern was selected taking into account only the mathematically useful surface of this horizontal area. The intersection plane was created as a 3 mm parallel plane to the previously created one.
Angles were measured using the axes of the created cylinders. The real angle between these axes and the plane created on the horizontal surface of the pattern was also measured.
Deviations were calculated as differences between the control reference distance and angles (measured using the CMM) and these reference parameters measured in digital impressions obtained with IOS.
Error in distance and angle measurements was measured in each of the reference parameters (reference distances and angles) and the mean and standard deviation of these errors were calculated. These calculations were repeated for each reference parameter and with each of the 3 IOS used. In addition, the results obtained with each IOS in each reference parameter were compared by applying the ANOVA variance analysis (P < .05). In order to apply this technique, the Levene test was previously used to check the homogeneity of the variances. Comparison of each measured parameter (distance and angle) was conducted using statistical analysis software (IBM SPSS Statistics 24, IBM Corp., Armonk, NY, USA).
RESULTS
After measuring the pattern with the CMM, reference distances were set at 32.405 mm for D12, 40.263 mm for D13, 40.622 mm for D14, and 32.804 mm for D15. Reference angles were set at 89°49′33″ for A1, −89°53′48″ for A2, −89°56′10″ for A3, −89°55′:50″ for A4, and −89°51′59″ for A5.
Concerning trueness, one-way ANOVA comparisons showed significant differences (P < .05) in all reference distances depending on the IOS used (Table 1). In order to discern the influence of each scanner, the scanners were compared in pairs, and results showed that these differences occurred especially when the Trios3 was involved. In all the distances that encompassed the equivalent of the digital impression of a quadrant including all incisors (D12, D13, and D14), significant differences were found comparing Trios3 with True Definition and Trios3 with iTero, while no significant differences were found between iTero and True Definition (P = .522 in D12, P = .907 in D13, and 0.764 in D14). In contrast, in D15 reference distance, the equivalent of a complete-arch digital impression, there were no significant differences comparing trueness achieved with Trios and True Definition (P = .141) or when comparing iTero with True Definition (P = .412). However, there were significant differences between Trios3 and iTero (P = .014).
Mean deviation ranged from 10 ± 7 µm to 42 ± 23 µm in D12 reference distance, from 16 ± 9 µm to 69 ± 34 µm in D13, from 21 ± 22 µm to 109 ± 44 µm in D14, and from 91 ± 63 µm to 174 ± 77 µm in D15. In D12, D13, and D15 reference distances, best mean deviation values were achieved with iTero while the larger mean deviation values were achieved in all cases using Trios3. Table 1 summarizes deviation values obtained with each IOS in each reference distance.
Concerning precision, one-way ANOVA comparison did not show significant differences (P > .05) comparing the three IOS. Significant differences occurred only in D12 reference distance and between Trios3 and iTero (P = .024). Mean precision values ranged from 10 ± 7 µm to 20 ± 11 µm in D12 reference distance, from 14 ± 13 µm to 28 ± 18 µm in D13, from 16 ± 18 µm to 33 ± 27 µm in D14, and from 52 ± 59 µm to 60 ± 58 µm in D15 reference distance. Table 2 summarizes precision values obtained with each IOS in each reference distance.
Concerning the trueness of angle measurements, one-way ANOVA comparisons did not show significant differences (P > .05) among the three IOS (Table 3). Contrasting the scanners in pairs, in general, significant differences were found in each measured angle. Nonetheless, no significant differences were observed between Trios3 and iTero in A1 (P = .874) and A5 (P = .660) reference angle or between Trios3 and True Definition in A3 (P = .103) and A4 (P = .668) reference angles.
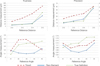
With regard to the measured angular deviations, it was found that while distance analysis clearly showed higher deviations as the scanning length increased, angle measurement analysis did not show the same evolution so clearly (Fig. 4). Minimum mean deviation values were measured in A1 reference angle (0.082 ± 0.068°); however, maximum mean deviation values were measured in A2 (0.475 ± 0.107°) and A3 (0.484 ± 0.127°) reference angles. All angle deviation values are shown in Table 3.
Contrary to significant differences observed upon analyzing the trueness concerning angle measurement, with precision, in general no significant differences were found - only in A3 reference angle between Trios3 and iTero (P = .032), and in A3 and A4 between iTero and True Definition (P = .027 in both).
In line with angle trueness, precision measurements did not worsen as the scanning length increased (Fig. 4). Best precision values were obtained in A3 reference angle assessed on 0.042 ± 0.024° and obtained with iTero, and the least precise values were obtained in A5 and with True Definition, assessed on 0.169 ± 0.126° (Table 4).
The distribution of trueness and precision data showed that distance error increased when the scanning area increased and that best results were achieved with iTero and True Definition (Fig. 5). Angle measurements did not show any conclusive data associated with the scanned arch length.
DISCUSSION
In this study, the accuracy of complete-arch digital impressions achieved with three intraoral scanners was assessed. The study was carried out following a new methodology and proved using in vitro tests.
The results obtained, similar to those obtained in previous studies, suggest that it is an applicable methodology for in vivo studies. This methodology was designed to measure the accuracy of scanners and to analyze the validity of results in certain clinical practices such as the fabrication of complete or partial restorations.
Many studies calculated the accuracy of IOS by superim-posing meshes obtained from these scanners, or with meshes obtained from industrial or desktop scanners.11222325262829 These superimpositions were carried out using best-fit alignment functions or minimizing distances criteria (specific functions to reverse engineering software). The results, obtained following these functions, provide important knowledge on the subject, especially for the manufacturers of scanners, although the use of scanners may present serious limitations in clinical practice when rehabilitations cover arch lengths longer than a dental piece.
The best fit functions align the meshes in order to achieve the minimum error; thus, this error is distributed as homogeneously as possible throughout the whole mesh. When the whole mesh represents a reduced space of the dental arch (from one to two teeth), as in the case of an impression to prepare a crown, the measurements of the resultant distributed error can be useful to establish whether or not the dental digital impressions are accurate enough. Measured error using best fit alignment functions could resemble marginal fit errors. However, in rehabilitations with implant restorations, it is preferable to know the error between fixation points rather than the homogeneously distributed error. According to this criterion, mesh alignments should be performed aiming for zero error at the first fixation point and measuring the accumulated error at other fixation points, instead of using best fit alignment processes that distribute the error and minimizes it in all the extension of the mesh. Some studies of IOS accuracy have followed these criteria of assessing distance or angulation errors between previously determined points.2324303637
The present study shows a methodology to assess the trueness and precision of digitally-acquired dental impressions using a measurement pattern. This pattern was provided with geometrically-helpful landmarks to easily measure the distance and angle errors, also used by other authors such as Van Deer Meer, Fukazawa, Güth, Zhang, or Kuhr.2425313738
On the other hand, many published IOS accuracy studies compared results achieved using IOS with results obtained by conventional procedures.11152728 However, these studies do not consider errors that conventional procedures can include. Impression materials can shrink, expand, or warp during or after removal from the mouth, resulting in inaccuracies. In addition, as in any type of process, each of the sub-processes carried out during conventional dental impressions can increase errors.111213 Therefore, one of the advantages of the proposed methodology is that instead of comparing the results with conventionally obtained models, they are compared with an accurately measured pattern that can be placed in the mouth. Thus, this methodology can be easily replicated in an in vivo study. Some studies have proposed similar methodologies based on the use of a pattern or externally-measured landmarks3037 However, the proposed methodology is valid for assessing the accuracy in different scanning lengths by measuring a once defined pattern. Thus, the deviation increase can be evaluated as the scanning length increases.
It is important to note that the proposed methodology has its limitations. The aim was to design a pattern that would fit in different mouths for later in vivo studies; for this, 5 volunteer arches were used. However, it is reasonable to assume that the pattern is not valid for all mouths and that in other cases the distances between the cylindrical abutments might not resemble implant or tooth positions. In addition, the shape of the pattern also limits the possibility of performing accuracy studies to the upper arch due to the difficulty of placing and maintaining the pattern placed in the lower arch. It is also worth noting that the study was performed using a pathology free and fully toothed model. The use of this same pattern in an edentulous case could influence the results since the pattern could provide the scanners with references to perform best fit unions. In addition to the obtained results, it should be noted that impression taking processes were performed using a model. It is assumed that the results presented would worsen in impressions in vivo due to the difficulties of obtaining them in real conditions.
In the trials conducted to test the methodology and establish the accuracy of IOS, distance and angle measurements showed different behaviors. Regarding distance analysis, results clearly showed that both trueness and precision worsened as the scanning area increased. These results also validate the proposed methodology for accuracy analysis as it confirms the conclusions obtained by previous studies (i.e. accuracy loss when increasing the length of dental arch to be scanned).1128 As shown in Fig. 4, deviations measured from digital impressions achieved with True Definition and iTero are similar, particularly when the impression reaches an archquadrant, including the incisors. In this distance, both IOSs achieved mean deviations below 25 µm and the maximum at 40 µm (95% Confidence Interval). With the Trios3 scanner, the measured maximum deviations reached 143 µm (95% CI) in D14 while mean deviation was 109 ± 44 µm. Considering previous studies that set maximum permissible errors at 100 µm, only those results obtained with iTero and True in a quadrant including all incisors are considered acceptable.7 Others have set maximum admissible errors at 150 µm, which makes acceptable digital impressions of complete arch achieved with iTero and True Definition (mean deviation of 91 ± 61 µm and 119 ± 61 µm and maximum in CI 95% of 146 µm or 147 µm, respectively).17 The highest inaccuracies were measured with Trios3, reaching a mean deviation of 174 ± 77 µm and a maximum of 233 µm (95% CI) in D14 distance.
The precision values showed a similar tendency to the deviations as shown in Fig. 4. Digital impressions were less precise as the scanning length of the arch increased, reaching values of maximum deviations in precision of 97 µm and 80 µm (Trios3 and True Definition in D15, respectively).
Angle measurement did not show such a clear trend due to the increase in the scanning arch length. However, Fig. 4 clearly shows how the best results in both trueness and precision were obtained with the iTero. The A1 and A5 reference angles did not give the best results despite there being no major differences among the scanners. However, in the angles A2, A3, and A4, the differences were greater and clearly showed better values for the iTero: deviation of 0.121 ± 0.065°, 0.099 ± 0.050°, and 0.117 ± 0.070° in A2, A3, and A4, respectively, and precision of 0.053 ± 0.034°, 0.042 ± 0.024°, 0.060 ± 0.030°, and 0.119 ± 0.067° in A2, A3, A4, and A5, respectively. It is worth noting that all measured angles gave deviation values below 0.4°, proposed by Andriessen as the maximum permissible.6
Despite the limitations of this in vitro study, results showed that IOS provide accurate digital impressions of a quadrant, confirming the conclusions obtained by previously published works related to the improvements implemented by IOS manufacturers to these devices.2439 Few years ago, IOS were even discouraged for complete arch impressions and there were no studies measuring their accuracy at various arch lengths. However, the most recent studies, as well as the present one, measure the accuracy of the full arch. Results also validate the proposed methodology as the values obtained for both trueness and precision are close to the published studies on the subject. The evolution of the error measured along the length of the arch also indicates logical and expected results showing worsening tendencies when the digitized arch length increases.
CONCLUSION
The current study shows that, at the time of performing the experimental part, the latest version of iTero provided greater accuracy in digital impressions of a dentate dental arch than the latest versions of Trios3 and True Definition. In addition, the proposed methodology was considered reliable to assess accuracy in terms of trueness and precision in vivo, considering both distance and angle deviations and in any dental arch length.








 XML Download
XML Download