

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Tuberculosis (TB) is a global health problem. According to the World Health Organization (WHO) report, there were an estimated 10.4 million new TB cases worldwide in 2015, of which 480,000 cases were multidrug-resistant TB (MDR-TB), and an additional 100,000 cases were rifampin (RIF)-resistant TB that were also newly eligible for MDR-TB treatment1. In Korea, isoniazid (INH) resistance rates were 9.9% in new patients and 24.1% in retreatment patients2. The rate of MDR-TB among new TB cases increased from 2.7% in 2004 to 2.9% in 20082, and there were 30,892 new TB cases in 2016, of which 852 cases were MDR-TB3.
It is important to quickly identify the results of drug susceptibility testing (DST) in patients at increased risk of drug resistance and to choose individualized treatment regimens based on DST profiles. Korean guidelines for TB, issued in 2017, recommend that genotypic RIF resistance should be treated as MDR-TB until conventional DST results are identified4. Early detection of drug resistance allows immediate and effective treatment, which improves the prognosis and prevents MDR strains from transmission as well as acquisition of additional resistance. Although conventional DST using liquid media culture has shortened the time to 2 weeks compared to solid media culture using Löwenstein-Jensen (LJ) medium, recent advances in molecular tools, such as the detection of mutations associated with drug resistance, have helped to detect drug resistance earlier. Based on this, the WHO recommended the use of molecular line probe assays (LPAs) for rapid detection of MDR-TB in 20165.
The GenoType MTBDRplus assay (MTBDRplus assay; Hain Lifescience, Nehren, Germany) is a rapid molecular diagnostic test that simultaneously detects the presence or absence of Mycobacterium tuberculosis and mutations causing resistance to specific drugs6. This assay is one of the commercial versions of LPAs that detect drug resistance to RIF and INH relying on specific probes immobilized on nitrocellulose strips. INH resistance is known to be mostly related with mutations in katG and inhA gene789. Mutations in katG have been found to be associated with a high-level INH resistance, while inhA mutations produce both low-level resistance to INH and high-level resistance to prothionamide (Pto), which is used for the treatment of MDR-TB1011121314. Cross-resistance to Pto may occur in patients who had received INH but had never been treated with Pto15, and the frequency of cross-resistance in Korea has been reported to be 50%16.
Currently, Pto resistance can only be detected by phenotypic susceptibility test; however, the result of this test is often questioned due to low reliability and reproducibility17. Therefore, verifying the presence of inhA mutation helps determine the use of Pto in cases of MDR-TB before conventional DST is confirmed. Nevertheless, few studies have reported the correlation between the results of the MTBDRplus assay and phenotypic DST for Pto resistance.
In this study, we sought to analyze the relationship between gene mutation pattern according to the MTBDRplus assay and phenotypic INH and Pto susceptibility by conventional DST in patients with mutations on katG or inhA genes.
Materials and Methods
1. Study population
This study retrospectively enrolled patients whose MTBDRplus assay results revealed katG or inhA gene mutations from September 2009 to October 2016 at a single tertiary referral center, Asan Medical Center, Seoul, Korea. Baseline characteristics at the time of diagnosis were gathered, including age, sex, physical examination findings, body mass index (BMI), and medical history (previous anti-TB treatment, diabetes mellitus, chronic liver disease, chronic kidney disease stage ≥2, respiratory disease, transplantation, human immunodeficiency virus infection, anti-tumor necrosis factor [TNF]-α therapy, and hematologic malignancy). The study was approved by the Institutional Review Board of Asan Medical Center (approval number: 2017-1012). The requirement for informed consent was waived due to the retrospective nature of the study.
2. Collection of specimens and drug susceptibility test
Specimens from lung (sputum, bronchial washing by bronchofibroscopy, and lung tissue by percutaneous needle aspiration) and other involved organs (cerebrospinal fluid, intestine, lymph nodes, pleural fluid, kidney, bone, and muscle) were included. All specimens were subjected to Ziehl-Neelsen staining for examination of acid-fast bacilli (AFB) on smear and culture using both solid (Ogawa medium; Korean Institute of Tuberculosis, Cheongju, Korea) and liquid (BACTEC 960 Mycobacterial Growth Indicator Tube; Becton Dickinson, Sparks, MD, USA) media. MTBDRplus assay was performed on AFB-positive specimens or clinical isolates in patients with increased risk of drug resistance. Cultured clinical isolates were subjected to conventional DST. Conventional DST was evaluated by the absolute concentration method with LJ media at the Korean Institute of Tuberculosis, a Supranational TB Reference Laboratory. Growth exceeding that of the control wells by >1% was considered to indicate drug resistance. A low-level resistance to INH was defined as resistance to 0.2 µg/mL but susceptible to 1 µg/mL of INH, while a high-level resistance was defined as resistance to INH of 1 µg/mL. Isolates were tested for resistance to RIF using concentrations of 40 µg/mL. The MTBDRplus assay was performed according to the manufacturer's instructions. The assay detects the presence or absence of wild-type (WT) and mutant DNA sequences in rpoB, katG, and inhA , which are known to be associated with RIF and INH resistance. There are 27 reaction lines comprising six control lines and 21 WT or mutation reaction lines (MUT) as follows: eight rpoB WT (codon 505 to 533) and four MUT bands (MUT1, D516V; MUT2A, H526Y; MUT2B, H526D; MUT3, S531L), one katG WT (S315 region), and two MUT bands (MUT1, S315T[AGC315ACC]; MUT2, S315T[AGC315ACA]), two inhA WT (WT1, positions −15 to −16; WT2, positions −8), and four MUT bands (MUT1, C15T; MUT2, A16G; MUT3A, T8C; MUT3B, T8A). A gene mutation indicates the presence of MUT band and/or loss of WT band.
3. Statistical analysis
Descriptive statistics were used to describe patient characteristics. Categorical variables were reported as counts and percentages and compared using the Pearson's chi-square test or Fisher exact test. Continuously measured parameters were reported as means±standard deviation and were compared using student's t-test. Statistical significance was indicated for p-values of <0.05. All statistical analyses were completed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA).
Results
1. Baseline clinical characteristics
In this retrospective study, the authors reviewed 206 patients whose MTBDRplus assay results revealed katG or inhA gene mutations. The most common type of infection was pulmonary TB (n=185, 89.8%) followed by disseminated TB (n=12, 5.8%) and extrapulmonary TB (total n=9, 4.4%; lymphadenitis, n=5; intestine, n=2; kidney, n=1; osteomyelitis, n=1). Specimens were obtained from sputum (n=185), bronchial washing (n=3), lung tissue (n=1), and other involved organs (lymph node, n=6; pleural fluid, n=4; cerebrospinal fluid, n=2; intestine, n=2; renal abscess, n=1; spine, n=1; muscle, n=1).
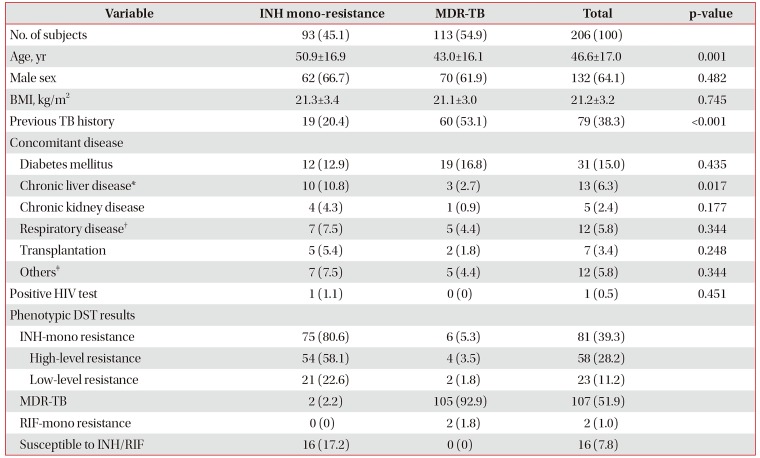
Stratifying by genotypic resistance to RIF, 54.9% isolates were found to be MDR and 45.1% were found to be INH mono-resistant by MTBDRplus assay (Table 1). Patients with MDR-TB were younger (43.0±16.1 vs. 50.9±16.9 years, p=0.001) and had a more frequent history of previous TB treatment (53.1% vs. 20.4%, p<0.001) than those with INH mono-resistance. There was no difference in sex and BMI. Comorbidities were similar in both groups except for chronic liver disease (2.7% in MDR-TB vs. 10.8% in INH mono-resistance, p=0.017).
2. Mutation patterns of katG and inhA genes by MTBDRplus assay
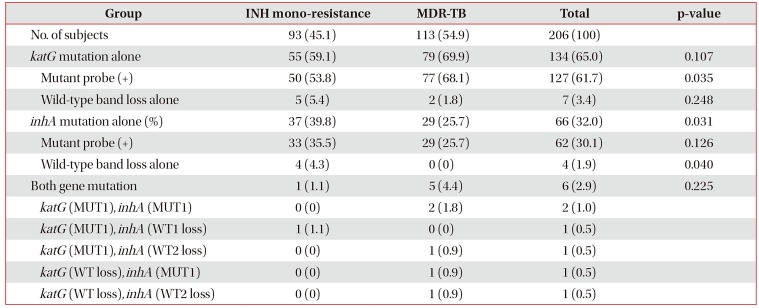
Table 2 shows mutation patterns of katG and inhA genes detected by the MTBDRplus assay. katG mutations were identified in 140 of 206 isolates (68.0%) and inhA mutations were identified in 72 of 206 isolates (35.0%). Except for six patients with both katG and inhA mutations, MDR-TB patients had more frequent mutations in katG than INH mono-resistant TB patients (69.9% vs. 59.1%, p=0.107), although this difference was not statistically significant. In contrast, MDR-TB patients had significantly less frequent inhA mutations (25.7% vs. 39.8%, p=0.031).
3. Correlation between phenotypic and genotypic susceptibility results based on mutation patterns of katG and inhA genes
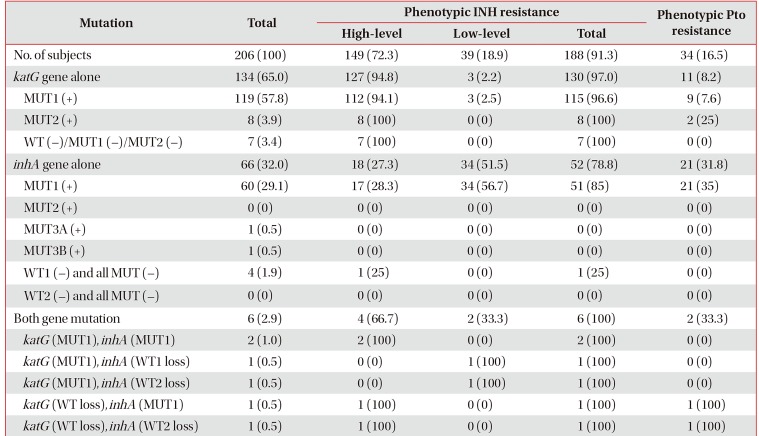
The concordances of the MTBDRplus assay and the conventional DST for the detection of INH and Pto susceptibility are shown in Table 3. Strains with isolated katG mutation presented phenotypic INH resistance in 97.0% and phenotypic Pto resistance in 8.2% of cases. Among the isolates with isolated inhA mutation, 78.8% were identified as phenotypic INH resistant and 31.8% as phenotypic Pto resistant. Of all genotypic INH resistant patients, 2.9% had mutations in both the katG and inhA genes, all of which were resistant to INH, and 33.3% were resistant to Pto. Except for six patients with both katG and inhA mutations, the presence of katG mutation presented high-level INH resistance in most cases (94.8%) while over half of the patients with inhA mutation (51.5%) showed low-level resistance. Of the 34 phenotypic Pto resistant isolates, 21 (61.8%) had an inhA mutation, 11 (32.4%) had a katG mutation, and two (5.9%) had both mutations.
Among the 134 strains with isolated katG mutation, MUT1 band was observed in 119 (88.8%) isolates, and positive MUT2 band and WT loss alone were observed in eight (6.0%) and seven (5.2%), respectively. Among the 66 isolates with isolated inhA mutation, the most common type was MUT1 (n=60, 91.0%), followed by WT1 loss alone (n=4, 6.1%) and MUT3A (n=1, 1.5%), and MUT3B (n=1, 1.5%). Among 127 strains with isolated katG mutant band (MUT1 or MUT2), 123 (96.9%) presented resistance to INH and 11 (8.7%) to Pto. Isolates with katG WT loss alone were all high-level INH resistant and Pto susceptible (n=7). Among 62 strains with isolated inhA mutant band (MUT1, MUT2, MUT2A, or MUT3B), 51 (82.3%) were INH resistant and 21 (33.9%) were Pto resistant. inhA WT loss alone was found in four isolates, of which one (25%) showed high-level INH-resistance and none showed Pto resistance.
Discussion
This study analyzed the relationship between gene mutation pattern and phenotypic INH and Pto resistance using the MTBDRplus assay. We analyzed 206 genotypic INH-resistant strains and found that 68.0% had a katG mutation and 35.0% had an inhA mutation. The presence of katG mutation presented high-level INH resistance in most case (94.8%), while over half of the patients with inhA mutation (51.5%) showed low-level resistance, which is consistent with previous studies101112. However, only 31.8% showed phenotypic Pto resistance in 66 patients with inhA mutations.
In our study, katG mutations were more frequent in MDR-TB isolates, and inhA mutations were significantly more frequent in INH mono-resistant isolates. According to previous studies, the frequency of S315T substitution in the katG gene is higher in MDR-TB than in INH mono-resistant TB1819 and might be related to the higher transmission capabilities of MDR-TB20.
Among the isolates with katG mutation, MUT1 (S315T) was the most common mutation. This is a transitional mutation G→C (AGC→ACC), resulting in the substitution of serine by threonine (S→T) in the amino acid chain. This S315T mutation has been found in up to 94% of the INH-resistant TB21, which is in agreement with our results. Among the isolates with inhA mutation, MUT1 (−15C→T) in the inhA promoter was the most common mutation. This mutation is found in up to 35% of INH-resistant and 55% of Pto-resistant TB22, which is also in agreement with our results.
Phenotypic Pto resistance presented in 8.2% of isolated katG mutations and 31.8% of isolated inhA mutations. In phenotypic Pto resistant isolates, 61.8% had inhA mutation, which agrees with the results of previous studies. Vilcheze and Jacobs22 mentioned that the proportion of inhA mutations in Pto-resistant TB is 68% on average, suggesting that this is the main mechanism of Pto resistance in M. tuberculosis. Pto is a structural analog of INH used as a second-line drug in the treatment of MDR-TB. Both INH and Pto are classified as pro-drugs that need to be activated by different mycobacterial enzymes. INH is activated by the katG-encoded catalaseperoxidase23, and Pto is activated by the NADPH-specific flavin adeninedinucleotide–containing monooxygenase EthA, which is regulated by EthR24. Once activated, the mode of action of each drug is very similar such that the active forms of the drugs react with NAD+ to yield an INH-NAD or ETH-NAD adduct, which inhibits inhA, leading to disruption of mycolic acid biosynthesis and cell death22. Therefore, mutations at the inhA gene can cause cross-resistance to INH and Pto by resulting in the overexpression or modification of the inhA target2526. In addition to the inhA mutation, ndh mutation causes cross-resistance to both drugs2728, and ethA, ethR, or mshA gene mutation also results in Pto mutation22. Because inhA mutation is considered as the major mechanism of Pto resistance in TB as previously mentioned, the use of LPAs would help physicians to get information about the use of Pto as well as RIF and INH. Nevertheless, few studies have reported the correlation between the results of the MTBDRplus assay and phenotypic DST for Pto resistance. Machado et al.25 examined 17 MDR-TB isolates and found that the presence of a mutation in the inhA regulatory region together with a mutation in the inhA coding region can lead to the development of high-level INH resistance and cross-resistance to Pto. Niehaus et al.29 sought to determine the proportion of patients who could potentially benefit from high-dose INH and who may be resistant to Pto. However, phenotypic Pto resistance was deduced from the inhA mutation because phenotypic DST was not performed. Rueda et al.30 examined the relationship between mutations and phenotypic resistance; however, they used whole genome sequencing, which is generally difficult for widespread use in clinical fields. In this study, only 31.8% showed phenotypic Pto resistance in 66 patients with inhA mutations, suggesting that Pto may be selected as one of MDR-TB regimen in patients with inhA mutation detected by MTBDRplus assay until phenotypic DST confirms Pto resistance. There could be two main speculations for the discrepancy between our hypothesis and the results. First, the low reliability and reproducibility of conventional DST of Pto might be the cause of the discrepant results17. Secondly, other compensatory mechanisms might play a role in maintaining Pto susceptibility in M. tuberculosis strains. Tan et al.31 found that mutations in the promoter region of inhA and inhA gene in Pto-susceptible isolates were different from those in Pto-resistant isolates, and these mutations are more likely to appear together with other mutations in Pto-resistant isolates. They suggested that these mutations may show cumulative effect on increasing minimum inhibitory concentration values of M. tuberculosis against Pto. We also speculate that mutations in specific parts of inhA may not affect Pto susceptibility.
Although the number of cases in this study was small, isolates with katG WT loss alone were all high-level INH resistant, while isolates with inhA WT loss alone were INH-resistant in only 25% of cases. Han et al.32 found one of 144 isolates showed low-level INH resistance with ahpC mutation confirmed by other LPA (AdvanSure MDR-TB GenoBlot assay), which revealed susceptibility to INH by conventional DST. The authors interpreted that the discrepancy might result from false positive of LPA, low-level resistance suppressing growth of M. tuberculosis at 0.2 µg/mL of INH, or hetero-resistance in which susceptible and resistant strains coexist. Therefore, in the case of genotypic INH resistance with isolated inhA wild type loss, we recommend that the possibility of an INH susceptible strain should not be ruled out before the final phenotypic DST results are obtained. None of four patients with loss of WT inhA band alone showed Pto resistance. Due to the small number of subjects and the absence of gene sequencing data, we could not draw any conclusion from this data. Further studies are needed to reveal the real meaning of this finding.
This study has several limitations. In patients with discrepant results between conventional and molecular DST, gene sequencing, a gold standard method of molecular test, was not performed. The phenotypic DST of second-line drugs such as Pto is considered as an unreliable test, but this test, as a gold standard method, was compared to MTBDRplus assay results. Finally, even though we enrolled a large number of isolates with katG or inhA mutations, the number of isolates with inhA WT loss alone was too small to draw any firm conclusion.
The katG and inhA mutations detected by MTBDRplus assay are good indicators of phenotypic INH resistance. However, only about one-third of inhA mutations revealed phenotypic Pto resistance, suggesting that Pto may be selected as one of MDR-TB regimen in patients with inhA mutation detected by MTBDRplus assay until conventional DST confirms phenotypic Pto resistance. We suggest that the reporting of detailed mutation patterns of MTBDRplus assay would be important for clinical practice, rather than simply presenting the resistance or susceptibility results.
 XML Download
XML Download