

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sarcoidosis is an inflammatory disease of unknown cause characterized by the presence of noncaseating granulomas1. The etiology of the disease remains unclear. However, because the lungs, eyes, and skin are commonly affected, the search for environmental causes has centered on exposure to airborne antigens2. The results of the U.S. study, ACCESS (A Case Control Etiological Study of Sarcoidosis), suggest a causal relationship between occupational exposure to insecticides, pollution, and mycobacteria, and the disease3.
The annual incidence varies widely throughout the world, probably because of differences in environmental exposure, surveillance methods, and predisposing human leukocyte antigen alleles. The highest annual incidence has been observed in northern European countries (five to 40 cases per 100,000 people). In Japan, the annual incidence is one to two cases per 100,000 people4.
In South Korea, there have been two national surveys56 by the Korean Academy of Tuberculosis and Respiratory Diseases (KATRD). The peak incidence in both surveys was in the 30 to 39 year age group, and the ratio of male to female cases was 1:1.5–2. Although the incidence is increasing, it is still considered a rare disease, with less than one case per 100,000 people in South Korea.
Since the introduction of endobronchial ultrasound (EBUS)–guided transbronchial needle aspiration (TBNA) biopsy of mediastinal lymph nodes, the incidence of confirmed sarcoidosis is expected to have increased. We investigated clinical features of sarcoidosis diagnosed from 1996 to 2014 in two university-affiliated hospitals covering the Gwangju and Jeonnam areas of South Korea. The aim of this study was to survey the clinical characteristics and prognosis of patients with sarcoidosis.
Materials and Methods
Sarcoidosis of the lungs, and sarcoidosis of the lungs and lymph nodes have been classified according to the International Statistical Classification of Diseases and Related Health Problems (ICD-10)7 using codes D.86.0 and D.86.2, respectively. Electronic medical records at Chonnam National University (CNU) Hospital and CNU Hwasun Hospital (CNUHH) were searched for confirmed disease codes D.86.0 and D.86.2.
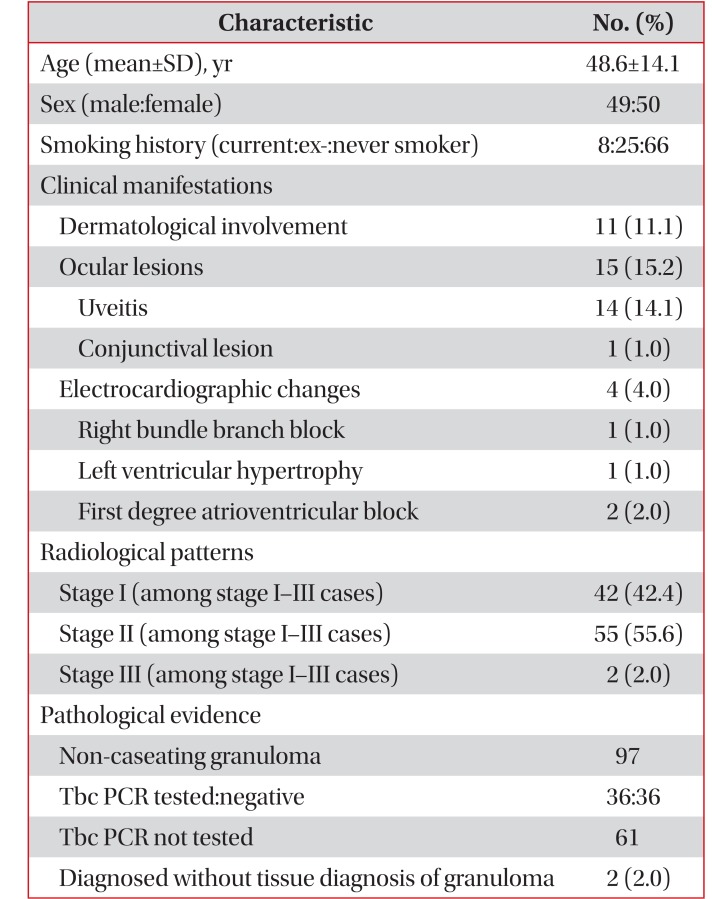
A diagnosis of sarcoidosis is established on the basis of compatible clinical and radiological findings, and by histological evidence of noncaseating epithelioid-cell granulomas in the absence of organisms or particles. As shown in Table 1, cases were selected using a combination of clinical, radiological, and pathological evidence. Of 115 cases with the relevant disease codes, 16 cases were excluded, as they had not been confirmed pathologically or had no definitive clinical features of sarcoidosis.
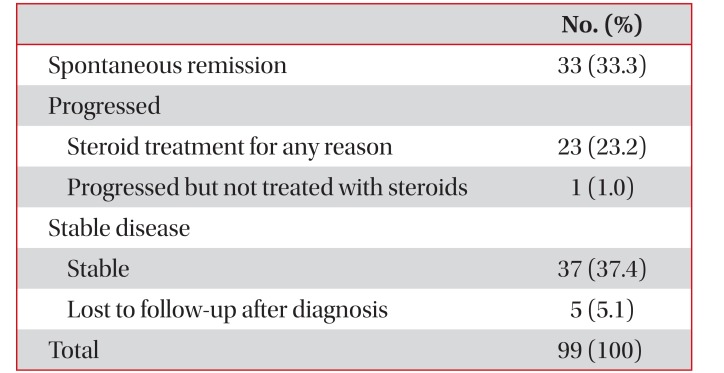
The clinical course after diagnosis was classified as remission, stable, or progressive disease, according to radiological changes or clinical manifestations, such as dermatological or ocular lesions. Clinical courses are summarized in Table 2.
Numerical data were expressed as mean±standard deviation (SD). Frequencies were represented as numbers and percentages. The duration from diagnosis to confirmed remission or disease progression was calculated by the Kaplan-Meier method and expressed as a median with a 95% confidence interval (CI). We estimated the median follow-up time using the reverse Kaplan-Meier method, by changing the event indicator from remission or progression to censoring8. Data were analyzed using IBM SPSS Statistics version 21.0 (Armonk, NY, USA).
Results
We found 99 patients with confirmed disease codes of sarcoidosis. The mean age of patients was 48.6 years and the peak incidence was observed in the 50 to 59 year and 30 to 39 year age groups. There was no sex difference and 66.7% of patients were never smokers.
Erythematous skin nodules or papules appeared in 11.1% of patients and ocular involvement was observed in 15.2% of patients (Table 1). Angiotensin converting enzyme (ACE) level was examined in 88 patients, and the mean ACE level was 68.1 U/L (SD, 31.7). Of the 85 patients whose serum calcium was checked, the mean serum calcium level was 9.29 mg/dL (SD, 0.53).
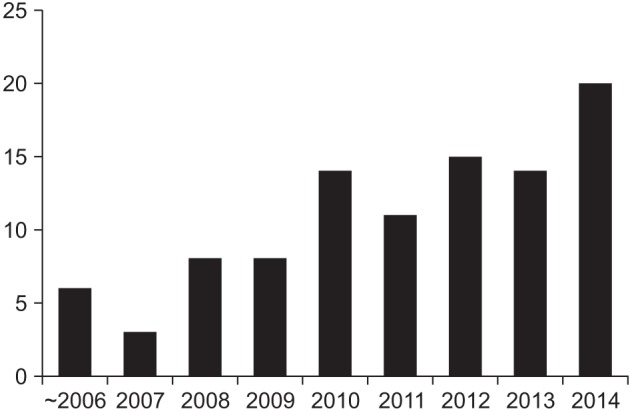
The annual numbers of diagnosed cases are shown in Figure 1. Only nine patients were diagnosed with sarcoidosis before 2008, while the remaining 90 patients were diagnosed from 2008 onward, after the introduction of EBUS-TBNA. Since 2008, the annual number of newly diagnosed sarcoidosis cases has increased, the highest number having been recorded in 2014.
Most patients (75.8%) were diagnosed by EBUS-TBNA, followed by mediastinoscopic biopsy (13.2%), and open surgical biopsy (5.1%); two patients were diagnosed by clinical and imaging studies without tissue biopsy. There were no cases of positive polymerase chain reactions for Mycobacterium tuberculosis among 36 cases tested.
According to radiological studies at the time of diagnosis, prevalence for stages of sarcoidosis was as follows: stage I (42.4%), stage II (55.6%), and stage III (2%). There was no case with radiologic findings of stage IV features such as fibrotic bands, bullae, hilar retraction, bronchiectasis, or diaphragmatic tenting.
The natural course of the disease is summarized in Table 2. After diagnosis, five patients were not followed up. Spontaneous remissions of disease was observed in 33 cases (33.3%), and stable disease in 42 (42.4%); progression was noted in 24 cases (24.2%) and systemic steroid treatment was initiated in 23 cases (23.2%).
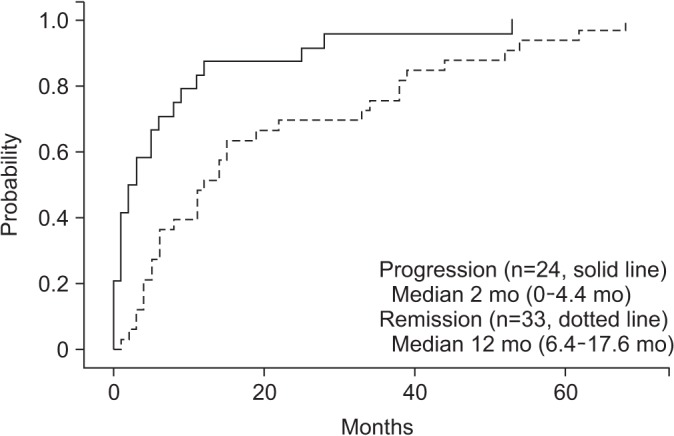
The median follow-up duration of the 99 cases was 46 months (95% CI, 37.5–54.5). Of the 42 cases with stable disease, the median follow-up duration was 23 months (95% CI, 14.3–31.7). Kaplan-Meier curves for patients with spontaneous remission (n=33) or progression (n=24) are shown in Figure 2. Median time to progression was 2 months (95% CI, 0–4.4) and median time to remission was 12 months (95% CI, 6.4–17.6).
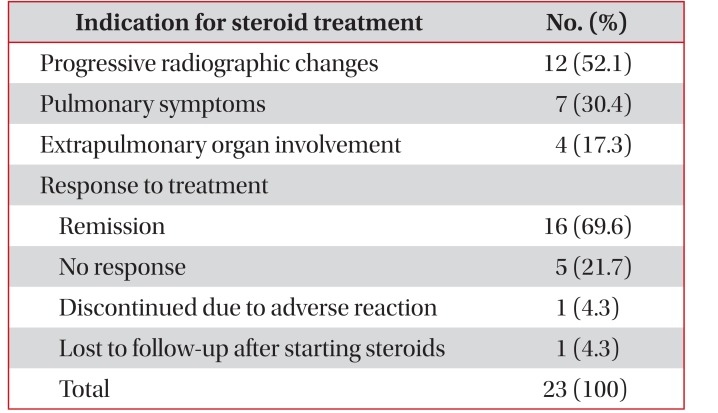
Table 3 shows indications for systemic steroid treatment. The most common reason for using steroids was progression of sarcoidosis on imaging studies, followed by worsening of subjective symptoms such as cough, sputum, or dyspnea. Systemic steroids were used in four patients due to involvement of extrapulmonary organs including the spleen (two cases), eyes (one case), and cervical lymph nodes (one case).
Of the patients treated with systemic steroids, 69.6% showed improvement. In five patients, the disease progressed despite systemic steroid treatment. Steroid treatment was discontinued in one patient due to moon face and epigastric pain, and another patient was lost to follow-up after initiation of steroid treatment. The median duration of steroid treatment was 5 months.
Discussion
Sarcoidosis affects people regardless of sex and occurs at all ages, although it usually develops before the age of 50 years, with the incidence peaking at 20 to 39 years3. It is unusual in children, teenagers, and those older than 70 years9. The preponderance of cases of sarcoidosis in females is consistent across racial and ethnic groups. In Scandinavia, the incidence in women appears to be bimodal, with one peak at 25 to 29 years of age, and another at 65 to 69 years of age10.
As this is a retrospective survey of cases from only two hospitals in a province, the data cannot reflect the true incidence of sarcoidosis in the region. Analysis of age distribution at diagnosis shows a bimodal distribution, with peaks at 30 to 39 years, and 50 to 59 years. In common with the results from other studies, the incidence decreases sharply in the 70-andolder age group. Unlike other surveys of sarcoidosis prevalence, there was no significant difference in incidence by sex.
Endobronchial and transbronchial biopsies have been the first-choice options for confirming sarcoidosis pathologically whilst avoiding a surgical biopsy. Endobronchial lesions are found in approximately 40% of patients with stage I disease and 70% of patients with stage II or III disease11. In sarcoidosis, endobronchial mucosal biopsies (EBB) are frequently positive and may increase the diagnostic yield, compared to transbronchial biopsies alone12. Transbronchial lung biopsy (TBLB) has a relatively high diagnostic yield (50%–75%) in patients who have bilateral hilar adenopathy or compatible lung parenchymal findings on high-resolution computed tomography (e.g., beaded or irregular thickening along bronchovascular bundles)1314. Moreover, bronchoscopy with transbronchial biopsy has a diagnostic yield of at least 82% when multiple lung segments are sampled15.
Since the introduction of the EBUS-TBNA technique, the diagnostic yield of bronchoscopy for sarcoidosis has increased. In a randomized trial comparing EBUS-TBNA versus conventional TBNA in combination with EBB and TBLB, EBUS-TBNA showed the highest diagnostic yield for sarcoidosis. Adding EBUS-TBNA to TBLB significantly enhanced the diagnostic yield for sarcoidosis16. Recently, another retrospective study compared the diagnostic yield of EBUS-TBNA and TBLB in 653 patients with suspected stage I and II sarcoidosis17. The overall diagnostic accuracy for EBUS-TBNA was 84%, and higher than TBLB.
Our study shows a considerable increase in the number of cases since 2008. Among other important reasons, it is suspected that the introduction of EBUS-TBNA in 2008 greatly improved diagnosis of sarcoidosis; EBUS-TBNA was the predominant method of diagnosis in 75.8% of all diagnosed cases.
ACE levels were not reliable diagnostic indicators since they were markedly elevated in only a fourth of patients in the present study. Sarcoidal granulomas produce ACE, and ACE levels are reported to be elevated in 60% of patients with sarcoidosis. However, the value of serum ACE levels in diagnosing or managing sarcoidosis remains controversial. As a diagnostic tool, measurement of serum ACE levels lacks sensitivity and specificity. For example, the positive and negative predictive values were only 84% and 74%, respectively, in one study18.
As sarcoidosis involves multiple organs, clinical symptoms are diverse. In previous national surveys in South Korea19, the frequency of organ involvement was as follows: lungs (87.1%), skin (30.7%), eyes (14.2%), and peripheral lymph nodes (12.9%); the heart was rarely involved.
Skin involvement is common (occurring in 25% to 35% of patients with sarcoidosis), and is often overlooked or misinterpreted, given the variability of the lesions. Macules, papules, and plaques may arise as single, isolated lesions or in crops. Lesions commonly involve the nape of the neck and upper back, extremities, and trunk, and may appear in scars and tattoos4. In our study, the incidence of skin lesions was only 11.1%, suggesting that skin involvement might have been underestimated.
The prevalence of ocular involvement observed in clinicbased cohorts has varied widely, from less than 10% in Finland to over 70% in Japan20. Anterior uveitis is the most common manifestation, occurring in 65% of patients with ocular involvement; posterior segment involvement is reported to occur in nearly 30% of the patients with ocular sarcoidosis21. In this study, the incidence of ocular involvement was 15.2%, mostly in the form of uveitis.
Chest radiographs in patients with sarcoidosis have been classified into four stages: stage I, bilateral hilar lymphadenopathy without infiltration; stage II, bilateral hilar lymphadenopathy with infiltration; stage III, infiltration alone; and stage IV, fibrotic bands, bullae, hilar retraction, bronchiectasis, and diaphragmatic tenting. These so-called stages represent radiographic patterns and do not indicate disease chronicity or correlate with changes in pulmonary function. Most studies report the predominance of stages I (40%–65%) and II (20%–40%)19. Our study also showed similar trends in stage distribution.
Within a decade of diagnosis, two thirds of patients with sarcoidosis generally have a remission, with few or no consequences; remission occurs within 3 years for more than half of patients. Up to a third of patients have unrelenting disease, leading to clinically significant organ impairment4. In our study, spontaneous remission occurred in approximately one third of patients, with a median duration of 12 months, while another third remained stable. It was unclear whether the patients in a stable state would have had spontaneous remission or whether the disease would have progressed. However, since many patients in a stable state did not return to the hospitals after diagnosis, and their median follow-up duration was less than 2 years (23 months), there is a possibility they underwent spontaneous remission during the follow-up period.
Although a large number of patients with sarcoidosis undergo spontaneous remission or have a benign clinical course, no clear predictors of spontaneous remission or disease progression have been identified. Oral glucocorticoid therapy generally improves symptoms (e.g., cough and dyspnea) and radiographic abnormalities, at least initially. However, assessment of the benefits of glucocorticoid therapy in the treatment of sarcoidosis remains problematic. The marked variability in presentations and clinical courses make it difficult to evaluate whether an apparent response to therapy reflects a treatment effect or the natural course of that patient's disease2223. In our study, 69.6% of the patients treated with systemic steroids responded and showed an improvement in disease.
In conclusion, following the introduction of EBUS-TBNA, the number of newly diagnosed sarcoidosis patients has increased. Clinical features of sarcoidosis are similar to those reported previously. Spontaneous remission occurred in approximately one third of cases, while one fourth of cases required systemic steroid treatment.
 XML Download
XML Download