

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Multidrug-resistant tuberculosis (MDR-TB) is by definition resistant to isoniazid and rifampin and consequently requires complex therapy of five or more medications of considerable toxicity but less potency and administered, in most cases, for more than 2 years1. Globally, MDR-TB treatment outcomes remain poor, largely due to lack of diagnosis, delay in treatment initiation, access to an expanded formulary of active drugs and the considerable public health infrastructure necessary to assist a patient to treatment completion2. While treatment outcomes for MDR-TB in the United States have been reported as equivalent to drug-susceptible tuberculosis (TB) in some settings, the total cost of treating a MDR-TB patient has been estimated at $134,000, and as high as $430,000 for extensively drug-resistant (XDR)-TB, with the majority of patients requiring medication changes during therapy3,4,5.
In Virginia, MDR-TB cases usually comprise less than 1% of total TB annually and patients are managed with expert guidance from state TB consultants. Increasingly state TB consultants have practiced therapeutic drug monitoring (TDM) for medications in the MDR-TB regimen to assure adequate peak concentrations and minimize toxicity. Given the association of suboptimal drug concentrations with poor outcome for drug-susceptible TB6,7, Virginia has operationalized the use of TDM for slow responders to drug-susceptible TB treatment and for all TB patients with diabetes8. Similar state guidelines have not been applied to TDM for MDR-TB. While some centers regularly employ TDM for MDR-TB management9, actual reports of TDM usage for second-line medications remain limited. Therefore, we sought to describe TDM usage patterns and pharmacokinetics for patients treated for MDR-TB in Virginia from 2009-2014, and relate these findings to emerging trends in management.
Materials and Methods
The state TB registry was searched for all patients with Mycobacterium tuberculosis and microbiologically confirmed resistance to isoniazid and rifampin from 2009-2014. Surveillance data were retrieved and included demographics (age, sex, and country of origin), comorbidities including human immunodeficiency virus and diabetes, prior TB history, and the anatomic focus of the current TB episode. Additional drug resistance results by conventional phenotypic drugsusceptibility testing was performed per routine at the state TB laboratory for isoniazid, rifampin, streptomycin, pyrazinamide, and ethambutol, but second-line drug susceptibility was performed at one or more referral laboratories. Outcomes reported were completion of treatment, time to sputum culture conversion to negative (in months for subjects with pulmonary MDR-TB), relapse following treatment completion, acquisition of new drug resistance in a TB strain previously susceptible to a given drug, and death from any cause during treatment. Information about medication-related adverse events was obtained from the state TB medical consultants.
All TDM required authorization by the state TB control office and laboratory report forms were thus reflective of actual usage patterns for each patient. The standard procedure for TDM was for patients to be given their daily dose of TB medications in the morning while fasting and then observed for 2 hours, during which they were restricted from eating or drinking. At 2 hours after medication administration (C2hr), venous blood was collected and serum was separated before transport on dry ice to the referral laboratory. All TDM was performed at the Infectious Diseases Pharmacokinetics Laboratory at the University of Florida with validated high-performance liquid chromatography, gas chromatography-mass spectrometry or colorimetric assays. The drug concentrations were compared to the expected C2hr ranges as an estimate of peak concentration10. For patients in whom TDM was performed for para-aminosalicylic acid, the concentration was checked at 6 hours given the known delayed peak. Some clinicians elected to check C6hr TDM as a marker of delayed absorption for other medications in the regimen and when available these results were compared to the C2hr result from the same day to calculate the Cmax.
Data analyses were largely descriptive with simple proportions reported and for continuous variables, means with standard deviation or medians with minimum and maximum values when appropriate. For the medications most frequently utilized for TDM, exploration of a demographic variable's association with a C2hr value below the expected range was calculated by univariable regression. The study was approved by the Institutional Review Boards at the Virginia Department of Health and the University of Virginia.
Results
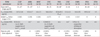
During the study period, 10 patients with MDR-TB were initiated on treatment. The mean age was 36.4±16.4 years, 6 (60%) were male, and all were foreign born (Table 1). Three patients had pre-XDR-TB including a 76-year-old man with cavitary pulmonary disease and a M. tuberculosis isolate with additional ofloxacin resistance (patient 7), a 32-year-old woman with non-cavitary pulmonary disease and an isolate with additional resistance to all injectable agents (patient 2), and a 42-year-old man with non-cavitary disease and kanamycin resistance but retained susceptibility to other injectable agents (patient 8). All patients were ultimately treated with regimens of ≥4 active drugs based on drug-susceptibility testing (Table 1). Of the five patients identified in 2012, four were genotypically linked to two separate clusters.
1. TDM usage
Eight patients (80%) had TDM for at least one drug performed (maximum 6 drugs). Patients without TDM either died early (patient 2) or were transferred out of care (patient 6). Initial TDM was performed at a median of 6.5 weeks (minimum 2, maximum 14 weeks) after MDR-TB treatment initiation. Of the eight subjects with initial TDM, six (75%) had at least one follow-up concentration performed, though for some medications repeat testing was performed without dose adjustment (Figure 1). All dose increase or decrease led to C2hr increase or decrease respectively in subjects with follow-up samples, while follow-up C2hr concentrations were not significantly different if the dose was unchanged (Figure 1). Limited 6-hour concentrations for delayed absorption generally supported the 2-hour result (Table 2). For the medications most frequently checked (cycloserine, capreomycin, and moxifloxacin), no demographic characteristic was associated with a C2hr value below the expected range.
2. Low dose cycloserine
Cycloserine was the most common medication for which TDM was performed, tested in seven (88%) of patients with TDM. Cycloserine C2hr values were below the expected range in 4 (57%) of initial concentrations (mean, 16.6±10.2 µg/mL) (Table 2). Five patients were treated with a 250 mg daily dose despite some recommendations of initial bid dosing or total daily doses up to 750 mg11. All C2hr concentrations below the expected range were in patients on daily dosing, yet only two patients had doses subsequently changed (to 250 mg twice a day). No patient on cycloserine was reported to have experienced psychosis.
3. Later generation fluoroquinolone use
Moxifloxacin was used in patients with fluoroquinolone-susceptible MDR-TB at 400 mg daily, and in only one patient (20% with TDM performed for moxifloxacin) was the initial C2hr value below the expected range (mean, 3.2±1.5 µg/mL) (Table 2). For the patient with the low initial C2hr (0.68 µg/mL, patient 5), following dose increase to 600 mg daily, the C2hr increased to within the expected range (4.7 µg/mL). Additionally, quantitative susceptibility by minimum inhibitory concentration (MIC) and pharmacodynamic testing (plasma TB drug activity [TDA]) were performed for two patients managed at the University of Virginia12. While each patient was treated with a moxifloxacin based regimen, the ratios of moxifloxacin C2hr/MIC were 35.3 and 17.4, while the corresponding TDA for each patient (higher value is more killing from patient's own plasma against their M. tuberculosis isolate) was 3.0±0.18 and 2.47±0.05, respectively. These values were both in excess of a 2-log killing within the TDA assay, suggestive of good pharmacodynamics12.
4. Pharmacokinetic variability of the injectable agent
Capreomycin was the most commonly used injectable agent, given at a standard 15 mg/kg dose (maximum 1 g), and found to be below the expected peak range in three (60%) of those tested with a wide distribution of values (mean, 21.5±14.0 µg/mL) (Table 2). However, the time to peak concentration of capreomycin is expected 1 hour after intramuscular injection or at the end of intravenous infusion, thus C2hr values may underestimate true peak. The second C6hr sample, which can more accurately be used by the reference laboratory to estimate clearance and half-life, was collected in only two patients but was supportive of a peak concentration below the expected range (calculated Cmax of 25.12 µg/mL in patient 2 and 31.84 µg/mL in patient 5, with calculated trace trough values for each).
5. Linezolid as an emerging second-line option
Linezolid was used in the patients with pre-XDR-TB (patients 2, 7, and 8). Initial C2hr values were within the expected range for both patients on 600 mg daily dosing, and low in the patient receiving 400 mg daily dosing (patient 7). A linezolid trough value was checked in only one patient (immediately before daily drug administration) and found to be undetectable. There were no reports of linezolid toxicity. Patient 7 died while on linezolid but this was deemed possibly related to TB and not a medication side effect.
6. Treatment outcomes
One patient elected transfer back to their home country within the first month of treatment and outcome was unknown (patient 6). Of the remaining nine, seven (78%) were either cured or are clinically improved and completing therapy (patient 10). The median time to sputum culture conversion among subjects with pulmonary TB was 3 months (maximum 5). There were no documented cases of relapse or acquired drug resistance to date. In the subject with diabetes, anti-diabetic medications were not documented as given, and all medications checked for TDM were within the normal range. Of the two deaths, patient 2 had advanced acquired immune deficiency syndrome (CD4 count of 44 cells/mm3) and was not on antiretroviral therapy at the time of presentation, was obtunded with severe MDR-TB meningitis, and died within 1 month of presentation. In the other, patient 7, capreomycin and linezolid concentrations were below the expected range near the time of death and while the cause was uncertain, it was thought possibly TB related. The small sample size and lack of uniformity in TDM precluded any other association of pharmacokinetics with treatment outcome.
Discussion
Nearly all patients treated for MDR-TB in Virginia during 2009-2014 had TDM performed for at least one medication. Dosages were frequently modified based on estimated peak serum concentrations leading to predicted concentration change in follow-up testing. Overall, treatment outcomes remained compatible with national norms3, yet a more refined approach to TDM may limit over-testing and further maximize therapeutic gain.
For certain drugs, such as the injectable agent capreomycin, individual pharmacokinetic variability was common and TDM was used to balance adequate peak concentrations with toxicity. While prudent, we found opportunity for standardization of timing of TDM and recommend paired C2hr and C6hr samples to best inform estimates of true peak concentrations13. However, follow-up testing without dose change did not reveal any major differences with the initial testing and could reasonably be eliminated. Of note, initial use of capreomycin was felt advantageous in part because of the possible higher barrier to resistance compared to the other injectables for M. tuberculosis isolates with the rrs mutation (amikacin and kanamycin resistance) or the eis mutation (kanamycin resistance). The eis mutation in particular, observed in at least one patient in this cohort, has recently been proposed to enhance virulence14,15.
In contrast to the injectable agents, moxifloxacin concentrations often were within the expected range. Nevertheless, we would advocate for the continued use of routine TDM for moxifloxacin in concert with quantitative susceptibility testing given the drug's predictable concentration dependent bactericidal action and possibility of fluoroquinolone MIC values near the borderline of susceptibility16,17,18,19,20. As done for two cases in this cohort, evaluation of C2hr/MIC for moxifloxacin, or another later generation fluoroquinolone, is a clinically actionable strategy for optimization of a critical medication class in the treatment of MDR-TB.
Cycloserine was predominately employed at a low dose (250 mg daily) and TDM used to mitigate toxicity. This approach contrasts to a more commonly reported twice daily dosing with targets of 15 mg/kg or 750 mg total daily dose, such as recent report from Taiwan which confirmed a total daily dose correlation with peak concentration, as well as an event of psychosis in a patient with concentrations >35 µg/mL21. The low-dose approach did not appear to compromise treatment efficacy in our setting and minimized toxicity. One may consider reserving TDM only for patients with poor renal function, or if cycloserine is dosed twice daily such as in the setting of extensive drug resistance where other second-line oral options are unavailable.
Linezolid was employed in pre-XDR-TB patients with limited second-line drug options and despite the small number of patients appeared to be tolerated at a 600 mg daily dose (in no patient was linezolid stopped due to toxicity). We acknowledge the considerable side effect profile of linezolid and need for routine laboratory monitoring and clinical evaluation. Nevertheless, we harbor concerns about the use of lower dose linezolid given the report of acquired drug resistance in those receiving 300 mg daily for XDR-TB patients in salvage therapy and the documented poor circulating drug exposure, and supported by the lower C2hr values observed in the one patient receiving 400 mg daily dose in our cohort22. Thus, we would endorse TDM in any patient receiving linezolid for a prolonged period of MDR-TB treatment.
In contrast, pyrazinamide and para-aminosalicylic acid given at standard weight-based doses, were well absorbed and infrequently below expected peak ranges in our setting. Therefore we would defer pyrazinamide or para-aminosalicylic acid testing unless significant gastrointestinal disturbance is noted. We have observed minimal gastrointestinal side effects of para-aminosalicylic acid with the enteric coated granule form compared to ethionamide and the sustained release may offer a pharmacokinetic advantage23. Furthermore, paraaminosalicyclic acid has consistently been found to be more susceptible than ethionamide among MDR-TB isolates both in studies from the United States and internationally3,16,18.
Our analyses are limited by the small sample size and the observational nature of this report. Larger prospective studies of second-line drug pharmacokinetics, measured at multiple points within the dosing interval to provide actual area under the time concentration curve, may ultimately determine pharmacokinetic thresholds associated with outcome to be established for key drugs in the MDR-TB regimen (e.g., the fluoroquinolones). Yet in settings such as ours where TDM is already used for dose adjustment, such comparative studies could not adequately be performed.
Thus, we recommend a more formalized approach to TDM in the management of MDR-TB including routine use as early as possible after a tolerable and active regimen is established (we regularly employ the Molecular Detection of Drug Resistance [MDDR] service through the US Centers for Disease Control and Prevention [CDC] for rapid molecular drug-susceptibility) 24,25. Such an approach would include C2hr and C6hr testing for the injectable agent, fluoroquinolone and linezolid (if needed), and for cycloserine only when a standard dose approach is used. Meanwhile, follow-up TDM without dose adjustment appears largely unnecessary and may only add expense.


 XML Download
XML Download